After significant weight loss, two problems often sit on top of each other in the same part of the body. The first is loose abdominal skin that hangs in both a vertical and a horizontal direction. The second is a weakness in the abdominal wall at the navel, an umbilical hernia, that may have been present for years and become more obvious as weight came off.
As a Specialist Surgeon based at Maitland Private Hospital, I see this combination regularly in my practice in patients who have lost a large amount of weight, whether through bariatric surgery, weight loss medications, or sustained diet and lifestyle change. A Fleur de Lis abdominoplasty (tummy tuck) is a form of reconstructive surgery after major weight loss, and it is a significant surgical procedure. When a patient comes in for a Fleur de Lis abdominoplasty (tummy tuck) to treat that loose skin, an umbilical hernia is sometimes found at assessment or at the time of surgery. Where it is appropriate for that individual, the hernia can be repaired during the same operation.
 After Weight Loss 1")
 After Weight Loss 2")
This article explains what an umbilical hernia is, how I assess it in patients who have lost significant weight, and how repair fits into a Fleur de Lis abdominoplasty (tummy tuck). It also sets out the recovery, the scars, and the risks plainly, and it explains why the decision to do one operation or to stage the work is made for each patient at consultation rather than decided in advance.
What an Umbilical Hernia Is
 After Weight Loss 3")
A hernia happens when tissue from inside the abdomen pushes through a weak point in the muscle wall that is meant to hold it in. An umbilical hernia is the type that occurs at the navel, where the abdominal wall has a built-in point of weakness left over from where the umbilical cord passed through in the womb.
In adults the hernia shows as a bulge at or near the belly button. Many patients first notice it when they cough, sneeze, strain, or lift something heavy, because raising the pressure inside the abdomen pushes the contents out further. The bulge may soften or disappear when lying down and become more obvious when standing. The contents of the hernia sac are usually fat from inside the abdomen, and sometimes a small portion of bowel.
Umbilical hernias are common. Published research indicates they make up a meaningful share of all adult abdominal wall hernias and are among the most frequently seen (1).
Why weight loss and pregnancy raise the risk
 After Weight Loss 4")
Anything that stretches or thins the abdominal wall over time can open up that point of weakness. Several lifestyle factors contribute, and the common ones include:
- A history of carrying significant weight, which stretches the abdominal wall for years before the weight comes off
- Pregnancy, particularly more than one, for the same reason
- Repeated rises in abdominal pressure from lifting heavy objects or a chronic cough
- Fluid in the abdomen
This is why I see umbilical hernias often in patients presenting after major weight loss. The wall was under load for a long time, and the defect at the navel is part of what that load leaves behind.
How hernias are grouped by size
Surgeons describe umbilical hernias by the size of the defect in the abdominal wall. As a rough guide, a defect under 1 cm is small, 1 to 4 cm is medium, and above 4 cm is large (1). Size matters because it influences how the hernia behaves, how it is repaired, and the chance of it coming back later.
A hernia that cannot be pushed back in, that becomes painful, hard, or discoloured, can be a sign that the contents have become trapped or that the blood supply is at risk. That is a situation that needs urgent medical assessment rather than planned surgery.
Symptomatic Versus Asymptomatic Hernias
 After Weight Loss 5")
Not every umbilical hernia behaves the same way, and not every umbilical hernia needs surgery. When I assess a patient I want to know whether the hernia is causing symptoms, how large the defect is, and whether it is changing over time, alongside their medical history. Those answers shape what I recommend.
Asymptomatic hernias
An asymptomatic hernia causes little or no trouble. It may be a small bulge that the patient barely notices, often slipping back in on its own or when pushed in, and showing mainly as an impulse when coughing. These are frequently picked up during a routine examination rather than because the patient complained of anything.
For small hernias that are not causing symptoms, watchful waiting is a recognised and reasonable approach rather than rushing to operate (2). The hernia is monitored, and surgery is considered if it grows or starts to cause problems. I do not treat a small, quiet umbilical hernia as an automatic reason for surgery on its own.
Symptomatic hernias
 After Weight Loss 6")
A symptomatic hernia makes itself known. Patients describe discomfort or pain, often worse with lifting, coughing, or straining, and the bulge tends to be larger and more persistent. Some hernias can no longer be pushed back in.
When a hernia is symptomatic, enlarging, or no longer reducible, surgical repair is worth considering. Leaving a progressing hernia carries a risk that a loop of bowel or fat becomes trapped, which can cut off the blood supply or cause a bowel obstruction. When the blood supply is lost this is called hernia strangulation. A hernia that suddenly becomes painful, firm, or discoloured needs urgent medical review, not a planned appointment.
How this fits with abdominoplasty
Many of the patients I see have an asymptomatic or mildly symptomatic umbilical hernia alongside a large amount of loose abdominal skin after weight loss. The skin is the reason they have come in. The hernia is found during that assessment. Whether the two are dealt with in one operation depends on the size and behaviour of the hernia and on the patient as a whole, which is covered further on.
Why the Belly Button (Umbilicus) Needs Attention After Weight Loss
 After Weight Loss 7")
The belly button (umbilicus) is not a free-floating piece of skin. It sits on a stalk of tissue that tethers it down to the abdominal wall. That anchoring point is exactly where an umbilical hernia forms, so in many patients the hernia and the belly button (umbilicus) are part of the same problem.
After major weight loss the belly button (umbilicus) changes in a particular way. It tends to look stretched and pulled downwards, with loose skin sitting around it and often hanging below it. This is different from the picture I see in some post pregnancy patients, where the navel can be more deeply set or funnelled. In the patient who has lost a large amount of weight, the issue is skin laxity. The skin and the belly button (umbilicus) have been stretched out and have not snapped back.
Why a belly button (umbilicus) procedure on its own rarely makes sense here
It is reasonable to ask whether the belly button (umbilicus) can simply be tidied up by itself. In a patient who has lost significant weight, the answer is usually no.
The stretched belly button (umbilicus) is surrounded by loose, redundant skin. Working only on the navel and ignoring that surrounding skin would leave the underlying problem untreated and the result would not sit well. The belly button (umbilicus) cannot be separated from the abdominal skin it is attached to. For this reason a standalone belly button (umbilicus) operation is rarely the right choice in this group.
The belly button (umbilicus) as part of the abdominoplasty
In an abdominoplasty (tummy tuck), the belly button (umbilicus) is handled as an integral part of the operation rather than an afterthought (3). As the loose abdominal skin is lifted and removed, the belly button (umbilicus) has to be carefully preserved on its stalk and then brought out through the redraped skin in a new, well positioned opening. The stalk itself can be freed and shortened to treat the stretching, and the navel repositioned so it looks settled rather than dragged down.
When there is also a hernia at that same spot, the repair sits within this part of the operation, because the surgeon is already working at the base of the umbilical stalk where the hernia lives.
The Fleur de Lis Abdominoplasty (Tummy Tuck) Explained
 After Weight Loss 8")
Standard abdominoplasty procedures remove loose skin through a single low horizontal incision and pull the remaining skin downwards. This is the usual tummy tuck (abdominoplasty) procedure most people picture. That works well when the excess skin runs mainly up and down. After major weight loss, the skin is often loose in two directions at once. It hangs down, and it is also slack from side to side, so pulling it down alone leaves a roll of horizontal looseness behind.
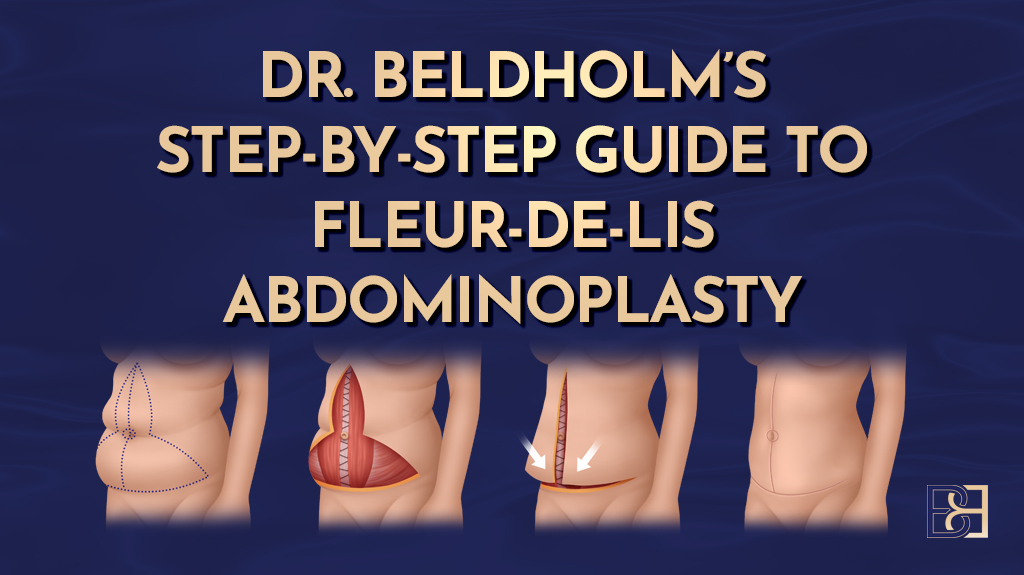
The Fleur de Lis abdominoplasty (tummy tuck) is designed for that situation. It treats laxity in both directions by combining two lines of skin removal.
How the incisions work
The operation uses two incisions that together form an inverted T:
- A horizontal incision low across the abdomen, similar to a standard abdominoplasty (tummy tuck), which removes the up and down excess
- A vertical incision running up the midline, which removes the side to side excess by drawing the skin in from both flanks
When I plan the vertical part, I have the patient standing and pull the loose skin together from side to side to judge how much can be removed. The vertical removal is widest beside the belly button (umbilicus) and tapers to a point higher up. The pattern of incisions resembles the Fleur de Lis, the stylised lily emblem the French term refers to (4).
The result targets the abdominal contour in both planes, which a traditional abdominoplasty using a single horizontal incision cannot do for this pattern of skin. The trade-off is a vertical scar up the midline in addition to the horizontal one, which is covered in the scars section below.
Muscle repair is assessed
 After Weight Loss 9")
There is a common belief that every tummy tuck (abdominoplasty) includes tightening of the abdominal muscles. That comes largely from pregnancy, and is more common in postpartum patients, where the abdominal muscles can separate down the midline, a condition called diastasis recti.
In patients who have lost significant weight without pregnancy, the underlying muscles are often intact and do not need repair. I assess each patient individually. If there are truly separated abdominal muscles (diastasis recti), muscle repair is done at the same time. If there is not, I do not add it for the sake of it. The main job in the weight loss patient is removing the loose skin and treating the belly button (umbilicus), not routinely tightening muscle.
Related approaches
For patients whose laxity extends across the upper and lower abdomen, the vertical removal can be extended, an approach sometimes described as a dual vector abdominoplasty. Whether a Fleur de Lis is the right choice, and how far the incisions need to run, depends entirely on the individual pattern of loose skin assessed at consultation.
Book your appointment online now
How I Repair an Umbilical Hernia During the Operation
When a hernia is repaired during a Fleur de Lis abdominoplasty (tummy tuck), the repair is woven into the operation rather than tacked on. The skin removal already takes me to the layer where the hernia sits, so the steps follow on from one another. Here is the sequence I follow.
Planning and marking
The operation is planned with the patient standing. I mark the horizontal incision low across the abdomen and judge the width of the vertical removal by drawing the loose skin together from each side. The position of the belly button (umbilicus) and any hernia bulge is noted at this point.
Anaesthesia
 After Weight Loss 10")
The procedure is done under general anaesthesia, so the patient is asleep throughout. The anaesthetic and airway are managed by the anaesthetist.
Incisions and lifting the skin
I make the horizontal and vertical incisions that form the inverted T, then lift the loose skin and fat off the abdominal wall as one flap.
The plane I work in matters. I dissect just deep to a layer called Scarpa’s fascia, which means Scarpa’s fascia stays within the flap that is removed, while the deeper fat and the lymphatic channels are left undisturbed on the abdominal wall. Keeping that deeper layer intact is associated with less fluid collecting afterwards (5).
Finding and freeing the belly button (umbilicus)
The belly button (umbilicus) stays attached to the abdominal wall on its stalk while the surrounding skin is lifted away around it. To keep track of the stalk during the operation I stitch a small marker to it, which lets me locate it reliably once the skin has been redraped. The stalk can be freed, trimmed, and shortened at its base to treat the stretching that weight loss has left behind.
Repairing the hernia
With the skin lifted, the defect in the abdominal wall at the base of the umbilical stalk is in clear view. This is the point where the surgeon identifies the size of the defect, which guides the repair. I return its contents (usually fat, sometimes a little bowel) back inside the abdomen, and close the defect.
- Smaller defects are closed directly with strong sutures
- Larger, recurrent, or complex hernias may need a mesh placed to reinforce the repair and lower the chance of it coming back (2)
- Throughout, the blood supply to the umbilical stalk is protected, because the belly button (umbilicus) depends on it to survive once it is brought back out (3)
Removing extra fat where needed
 After Weight Loss 11")
In some patients I use VASER, an ultrasound assisted form of liposuction (suction assisted lipectomy), to refine areas of stubborn fat at the flanks so the final contour sits evenly. This is judged case by case, not done routinely.
Closing and drains
Once the hernia is repaired and the belly button (umbilicus) prepared, the skin is redraped, the umbilicus is brought out through a new opening and stitched into place, and the incisions are closed in layers with the outer skin brought together last.
I place two surgical drains, one on each side, brought out through small exits near the hips. These closed suction drains draw off fluid and reduce fluid accumulation under the skin. The wounds are covered with a dressing at the end of the operation.
Combining Hernia Repair With the Abdominoplasty
 After Weight Loss 12")
When an umbilical hernia is found in a patient who is having a Fleur de Lis abdominoplasty (tummy tuck), it usually makes sense to repair it during the same operation. The hernia sits at the base of the umbilical stalk, which is already exposed once the loose skin is lifted. Repairing it there adds relatively little to an operation of this size, and from a medical point of view there is no real advantage in treating it as one of two separate surgeries on another day. Combining the hernia repair with the abdominoplasty in one surgical session keeps the work within a single recovery period. The patient avoids two separate surgeries and two separate recovery periods, and for a defect this size the combined surgery does not meaningfully change the recovery, which makes the combined procedure a reasonable approach.
The clear exception is an umbilical hernia that presents as an emergency. If a hernia becomes strangulated, a situation called hernia strangulation where the blood supply to the trapped contents is cut off, it needs urgent repair in its own right and cannot wait for planned surgery. In that situation the hernia is dealt with first and on its own, and any skin surgery is considered later.
Preparing for Surgery: Nutrition and Blood Tests
 After Weight Loss 13")
An abdominoplasty (tummy tuck) is a significant operation, and how well a patient heals afterwards depends in part on their nutritional state going into it. This matters more in patients who have lost a large amount of weight, because the same process that took the weight off often leaves gaps in protein and key vitamins and minerals behind. Correcting those gaps before surgery supports the healing process and recovery. Being at a stable weight before surgery also helps.
For this reason I run a full pre-operative blood panel on every post weight loss patient. It checks the blood count, iron studies, protein status using albumin, vitamin D, vitamin B12, folate, zinc, and a range of other markers, along with the standard pre-surgery and general health tests. Where the results show a deficiency, we treat it before the operation rather than discovering it during recovery. The results are copied to the patient’s GP, who manages long-term follow-up.
I keep the detailed nutrition guidance in a separate set of articles so it is not duplicated here. If you want to read further, I have written about protein needs after weight loss, the common nutritional deficiencies seen in this group, and the vitamins and supplements I use, and there is an overview of the pre-operative blood tests themselves. The short version is that preparation begins well before the day of surgery, and getting it right is part of making the operation a sound choice in the first place.
Recovery After the Operation
The recovery period after a Fleur de Lis abdominoplasty (tummy tuck) takes time and should not be underestimated. This is major abdominoplasty surgery, and it is the skin surgery that sets the recovery rather than the hernia repair. Here is what the recovery generally looks like, though the pace varies from patient to patient.
Hospital stay
 After Weight Loss 14")
Most patients stay in hospital for two to four nights. On the first day after surgery I want patients up and walking, even if only a short distance with help. Early movement is one of the most important things a patient can do, and I will come back to why below. A mild sore throat from the breathing tube used during the anaesthetic is common in the first day or so and settles on its own.
Drains and dressings
The two drains stay in until the fluid draining from them drops below a set level, which is usually somewhere between two and seven days. Some patients go home with a drain still in and have it removed at a follow-up visit.
 After Weight Loss 15")
The wounds are dressed with a PICO dressing, which uses negative pressure to support healing. I change this at around day seven and switch to a supportive tape called Hypafix over the scars.
Compression garment
 After Weight Loss 16")
A compression garment helps control swelling and supports the tissues while they heal. I ask patients to wear it full time for the first four weeks, then for about half the day for a further two weeks. Swelling tends to be worse later in the day, so daytime wear matters most, though there is room to adjust this for comfort in hot weather.
Pain and swelling
Many patients report real discomfort in the first week or two, managed with pain relief, and the recovery process eases steadily from there. Swelling and bruising are expected and take longer to settle. The abdomen can feel tight when standing upright at first, which is normal as the redraped skin settles.
Moving early and preventing blood clots
 After Weight Loss 17")
One of the risks after a long operation is deep vein thrombosis, a blood clot forming in the deep veins of the legs. Getting up and walking early is a key part of lowering that risk, which is why I encourage light movement from the first day. Other measures are used in hospital as well. I have written separately about deep vein thrombosis risk and prevention after body contouring surgery.
Returning to activity and work
 After Weight Loss 18")
Most patients with a desk-based job are back at work around four weeks. Those in physically demanding or manual jobs usually need six to eight weeks. Light walking can build up over the early weeks. In patients who did not need muscle repair, core exercises and squats can often resume from about four weeks, while those who had muscle repair take longer. I give specific guidance at follow-up. There is more detail in my article on exercise after abdominoplasty.
Follow-up
 After Weight Loss 19")
I review patients at four weeks, three months, six months, and twelve months after surgery. At the four week visit I hand care back to the GP for long-term management, along with the blood results and operation details. Recovery from the scars themselves continues well beyond these visits, which is covered next.
If something is not right
If you have a concern after hours, you call Maitland Private Hospital, where a nurse will triage the problem by phone. Anything needing a physical look goes to your local emergency department. For anything life-threatening, call 000. Maitland Private is not an emergency department.
Scars and How They Are Managed
 After Weight Loss 20")
A Fleur de Lis abdominoplasty (tummy tuck) leaves permanent scars, and being clear about that is part of planning the operation properly. The trade-off for treating loose skin in two directions is a scar that runs in two directions.
Where the scars sit
There are three scars to expect:
- A long horizontal scar low across the abdomen, which sits below the underwear line in most patients
- A vertical scar running up the midline, from the lower abdomen towards the breastbone, forming the inverted T
- A scar around the belly button (umbilicus) where it is brought out through the redraped skin
The vertical scar is the trade-off specific to the Fleur de Lis, and it is the reason this operation is chosen for the right pattern of loose skin rather than for everyone.
How scars change over time
Fresh scars are firm, raised, and pink or red. Over the following months they soften, flatten, and fade. This is a slow process. Most scars take twelve to twenty-four months to settle to their final appearance, and the result varies between patients depending on skin type, genetics, and how the wounds heal. Some people scar more than others, and that cannot be fully predicted in advance.
What helps
Once the wounds have healed, there are a few things that support better scar maturation:
- Silicone gel or silicone sheets used over the scars
- Scar massage once I clear you to start
- Protecting the scars and incision site from sun exposure, which can darken them while they are still immature
- Avoiding heavy strain on the healing wounds in the early weeks
I do not offer laser treatment for scars. The measures above, combined with time, are what I rely on. If a scar heals poorly, scar revision can be discussed later, once it has fully matured.
Risks and Possible Complications
 After Weight Loss 21")
Every operation carries risks, and a Fleur-de-Lis abdominoplasty (tummy tuck) with hernia repair is a major procedure. Part of giving consent is understanding what can go wrong. The following are the main risks and potential complications I discuss with patients. Not all of them are common, but all are possible.
Bleeding and fluid collections
- Bleeding under the skin, called a haematoma, can occur and occasionally needs a return to theatre
- Fluid accumulation under the skin flap, called a seroma, can also occur. Preserving the deeper fatty tissue and lymphatics during surgery lowers this risk, and the drains help as well (5)
Infection
 After Weight Loss 22")
Wound infection, also called surgical site infection, can occur after this abdominoplasty procedure, and it is one of the recognised complications in patients who have lost significant weight (4). Infections are usually managed with antibiotics, though a deeper infection can need further treatment.
Wound healing problems
The point where the vertical and horizontal incisions meet, the centre of the inverted T, is under the most tension and is the area most likely to be slow to heal or to separate slightly at the edges. Most of these settle with dressings and time, but they can lengthen recovery.
Hernia recurrence
A repaired hernia can come back. The risk factors include larger defects, smoking, a higher body weight, and poor wound healing. Using mesh for larger defects lowers the chance of recurrence compared with stitches alone (2).
Belly button (umbilicus) problems
The belly button (umbilicus) depends on its blood supply once it is brought back out through the skin. Rarely, that blood supply is compromised and part or all of the belly button (umbilicus) can have healing problems. Careful handling of the stalk during surgery is aimed at avoiding this.
Blood clots
 After Weight Loss 23")
Deep vein thrombosis, a clot in the deep veins of the legs, is a recognised risk after longer operations, and a clot can travel to the lungs. Early walking, and other measures used around the time of surgery, are aimed at reducing this risk.
Scarring and the need for revision
Scars are permanent and heal differently between patients. Some patients are left with a scar that is thicker or more noticeable than hoped, and a small number choose scar revision later. Other reasons for further surgery include treating a residual fold of skin or correcting a healing problem.
Anaesthetic and general risks
As with any operation under general anaesthesia, there are risks related to the anaesthetic itself and to a patient’s underlying health. These are assessed beforehand and managed by the anaesthetist.
Final Thoughts
 After Weight Loss 24")
An umbilical hernia and loose abdominal skin often turn up together in patients who have lost a large amount of weight, because the same years of stretch on the abdominal wall produce both. When a hernia is found in a patient having a Fleur de Lis abdominoplasty (tummy tuck), and it is not an emergency, it usually makes sense to repair it during the same operation, because the surgery is already working at that part of the abdominal wall.
What matters most is that the decision is based on careful assessment rather than assumption. The size and behaviour of the hernia, the pattern of loose skin, a patient’s nutritional state, and their general health all feed into the plan. Preparation before surgery matters, the recovery is significant, and there are real risks to consider.
My aim is to give patients an accurate picture of what the operation involves so they can make an informed decision about their own care.
References
- Coste AH, Jaafar S, Parmely JD. Umbilical Hernia. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2023.
- Henriksen NA, Montgomery A, Kaufmann R, Berrevoet F, East B, Fischer J, et al. Guidelines for treatment of umbilical and epigastric hernias from the European Hernia Society and Americas Hernia Society. Br J Surg. 2020;107(3):171-190.
- Hespe GE, Stepien DM, Sherif RD, Gilman RH. Umbilicoplasty in abdominoplasty: modifications for improved aesthetic results. Aesthet Surg J Open Forum. 2021;3(3):ojab025.
- Friedman T, O’Brien Coon D, Michaels J, Purnell C, Hur S, Harris DN, et al. Fleur-de-lis abdominoplasty: a safe alternative to traditional abdominoplasty for the massive weight loss patient. Plast Reconstr Surg. 2010;125(5):1525-1535.
- Repo O, Oranges CM, di Summa PG, Uusalo P, Anttinen M, Giordano S. Scarpa fascia preservation to reduce seroma rate on massive weight loss patients undergoing abdominoplasty: a comparative study. J Clin Med. 2023;12(2):636.