The umbilicus, or belly button, changes shape when the abdomen stretches with weight gain, and changes again when the skin is left loose after significant weight loss. By the time many of my patients reach me, the umbilicus sits deep within the abdominal wall, has been pulled out of position, or is hidden under an apron of loose skin.
In my practice, when I perform an abdominoplasty (tummy tuck) after significant weight loss, the umbilicus is part of almost every operation. As the loose abdominal skin is removed and the remaining skin is moved down, the umbilicus has to be repositioned so it sits where it normally sits on the abdomen. How I do that depends on the operation and on the condition of the umbilicus itself.
 in Post Weight Loss Abdominoplasty (Tummy Tuck) 1")
 in Post Weight Loss Abdominoplasty (Tummy Tuck) 2")
This article covers how weight gain and weight loss affect the umbilicus, how I reconstruct it across the different abdominoplasty operations I perform, when a standalone umbilicoplasty is an option, and how an umbilical hernia is managed at the same time. I have also set out the risks, the recovery, and what determines whether any of this is suitable for you.
Whether surgery is appropriate and which approach fits is decided individually at consultation. A GP referral is required before any consultation, and results vary from patient to patient.
What is the umbilicus?
 in Post Weight Loss Abdominoplasty (Tummy Tuck) 3")
The umbilicus (belly button, or navel) is a scar. Before birth, the umbilical cord runs from the baby to the placenta and carries the blood supply the baby depends on through pregnancy. After birth, the cord is cut, the small remnant dries and separates, and the skin heals over. What is left is the umbilicus, the first scar every person carries.
Whether the umbilicus heals as an “innie” or an “outie” depends on how the cord site closes and how the surrounding skin and abdominal wall develop. It is not a sign of anything having gone wrong. Once healed, the umbilicus is held to the abdominal wall by a short stalk of tissue. That stalk tethers it down and gives it its depth.
This anchoring matters for the rest of the article. Because the umbilicus is fixed to the abdominal wall rather than sitting loose in the skin, anything that stretches or loosens the abdomen, including weight gain and weight loss, pulls on it and changes how it looks.
How weight gain and weight loss change the umbilicus
 in Post Weight Loss Abdominoplasty (Tummy Tuck) 4")
The umbilicus does not change on its own. It changes because the abdomen around it changes. Weight gain and later weight loss act on it in different ways, and in many of my patients both have happened in turn.
How weight gain changes the umbilicus
As body weight rises, fat builds up in the abdominal wall and under the skin, and the abdomen expands. The umbilicus stays anchored to the abdominal wall by its stalk, so as the layer of tissue between the skin surface and the wall thickens, the stalk effectively lengthens. The umbilicus is drawn inward and downward into a deep, funnel-shaped pit.
While the weight is being carried, this produces a deep umbilicus set at the bottom of a thick abdominal wall. The opening can also widen or pull out of shape as the surrounding skin stretches. With a large overhang of abdominal skin and fat, the umbilicus can sit at the base of a deep fold, where it is hard to keep clean and dry. That can lead to skin irritation and recurrent infection in the fold, known as intertrigo, which is a practical problem rather than only a question of appearance.
How weight loss changes the umbilicus
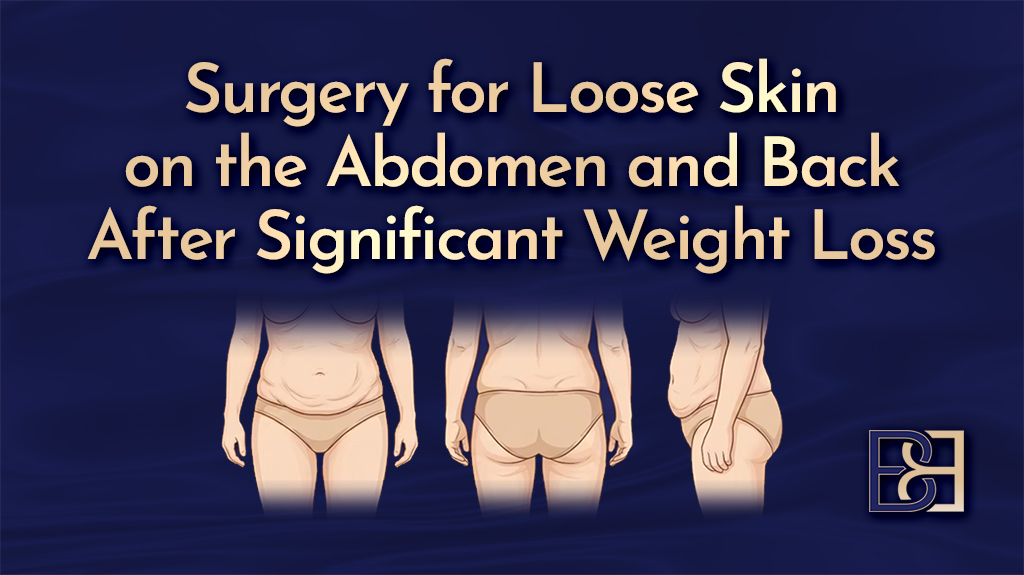
After significant weight loss, fat volume decreases, but the skin that stretched to hold it does not shrink back to the same extent. The result is loose, excess skin that hangs over the lower abdomen as an apron.
By the time patients reach me, they have usually already lost the weight, so this is the stage I see most often. The umbilicus is still tethered to the underlying abdominal wall, and as the loose skin is pulled down, so is the umbilicus. It commonly looks stretched and elongated and may sit off to one side. The stalk that lengthened while the weight was carried usually stays long. This matters at surgery because the length of the stalk and its blood supply affect how the umbilicus can be reconstructed, which I cover in more detail later.
Weight changes also raise the chance of an umbilical hernia, where tissue pushes through a weak point in the abdominal wall near the umbilicus. I deal with that separately below.
 in Post Weight Loss Abdominoplasty (Tummy Tuck) 5")
Umbilical shape varies from person to person
There is no single correct shape for an umbilicus. Shape and depth vary widely between people and are influenced by genetics, age, weight, previous pregnancy, piercings, and how the cord site healed at birth. Some umbilici are vertical, some horizontal, some round or oval, some deep and funnelled, and some protrude outward. All of these fall within normal variation.
 in Post Weight Loss Abdominoplasty (Tummy Tuck) 6")
Researchers have tried to describe this range in a structured way. Published research has set out a classification called SHAPE, which looks at the umbilicus across five features: its shape, any hood of skin above it, the surrounding fat, how much it protrudes and where it sits, and whether it has been pierced (1). A tool like this helps a surgeon accurately describe an individual umbilicus. It is not a standard that anyone needs to meet.
Is an outie belly button normal?
Yes. An “outie”, where the umbilicus protrudes rather than sits inward, is a normal variation. It is less common than an “innie”, but it is not a sign that something is wrong.
In babies, an outie is often caused by a small umbilical hernia, in which a small piece of tissue pushes out through the site where the umbilical cord attached. Most of these close on their own in early childhood, and the umbilicus settles inward. An outie that comes from the way the cord healed, rather than from a hernia, usually stays much the same through life.
In adults, a new or enlarging outie can be a sign of an umbilical hernia, particularly after weight changes or pregnancy. If the umbilicus has changed shape, become firmer, or is uncomfortable, it is worth having it assessed, because a hernia is a separate matter from how the umbilicus looks. I cover umbilical hernia further on.
The umbilicus in post weight loss abdominoplasty (tummy tuck)
In post weight loss patients, the umbilicus is reconstructed as part of almost every abdominoplasty (tummy tuck) I perform. It is not a separate add-on. It is a built-in step in the procedure because of how the loose abdominal skin is removed.
Why the umbilicus has to be repositioned
 in Post Weight Loss Abdominoplasty (Tummy Tuck) 7")
During an abdominoplasty, I lift the loose abdominal skin and fat off the abdominal wall, advance it downward, remove the excess, and close the lower incision. The umbilicus, though, is anchored to the abdominal wall by its stalk. It does not travel down with the skin.
 in Post Weight Loss Abdominoplasty (Tummy Tuck) 8")
To keep the umbilicus in place, I cut around it and dissect it down to the abdominal wall, so it stays attached there on its stalk. The abdominal skin flap is then lifted off the wall around the umbilicus and advanced downward, leaving the umbilicus sitting on its stalk. Once the skin is in its new position, I make a new opening at the correct level and bring the preserved umbilicus out through it, stitching it into place. This step is called umbilical transposition.
 in Post Weight Loss Abdominoplasty (Tummy Tuck) 9")
In post weight loss patients the umbilicus itself is usually stretched, so reconstructing it involves more than relocating it. After freeing the stalk, I trim the stretched, excess skin of the umbilicus. A stretched umbilicus also tends to be pulled outward and elongated rather than sitting recessed, so I shorten it at its base with sutures to tighten it and set it back into the abdomen.
 in Post Weight Loss Abdominoplasty (Tummy Tuck) 10")
If the umbilicus were pulled down with the skin instead, it would end up sitting too low on the abdomen and be pulled out of shape. Repositioning and reshaping it is what keeps it sitting recessed where the umbilicus normally sits.
Transposing the umbilicus, or creating a new one
 in Post Weight Loss Abdominoplasty (Tummy Tuck) 11")
There are two broad ways the umbilicus is handled.
- Transposition. The patient’s own umbilicus is kept on its stalk and repositioned through a new opening in the skin. This is the usual approach and preserves the original umbilicus.
- Neo-umbilicoplasty. A new umbilicus is constructed. I use this when the original umbilicus cannot be preserved, for example, if its blood supply is not reliable, if the stalk is too long or thinned after major weight loss, or if it has to be removed as part of the skin pattern being excised.
Blood supply is the key consideration. The umbilicus is fed through its stalk and its attachment to the abdominal wall, so that attachment has to be protected during surgery. In patients who have lost a large amount of weight, the stalk is often long, and the tissue thinned, which can make the blood supply less reliable. That is one reason I may choose to construct a new umbilicus instead. Published techniques exist for building a new umbilicus when this is needed (2).
How does this differ across the operations?
The same principle applies to the abdominoplasty operations I perform after weight loss, but the details vary with the skin pattern removed in each case.
Full abdominoplasty (tummy tuck). The umbilicus is cut around and transposed through a new opening in the advanced skin. This is the standard approach for a horizontal lower abdominal excision. See full abdominoplasty post weight loss.
 in Post Weight Loss Abdominoplasty (Tummy Tuck) 12")
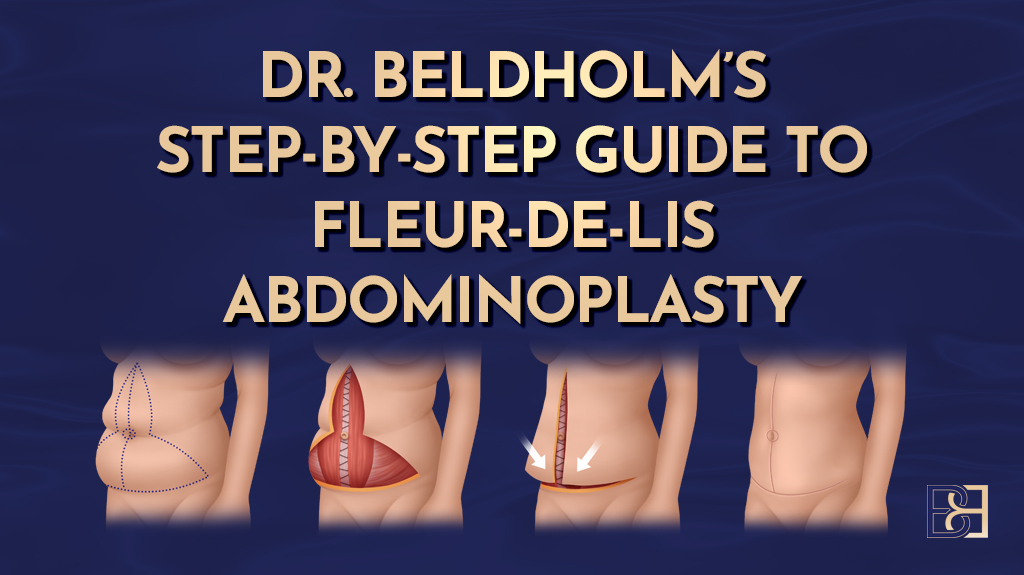
Fleur-de-Lis abdominoplasty. This adds a vertical midline excision to the horizontal one for patients with both vertical and horizontal skin excess. The vertical incision runs close to the umbilicus, which is preserved and transposed where possible, or reconstructed as a neo-umbilicoplasty if it cannot be kept. See Fleur-de-Lis abdominoplasty post weight loss.
 in Post Weight Loss Abdominoplasty (Tummy Tuck) 13")
Dual vector abdominoplasty. This combines a Fleur-de-Lis with the removal of upper abdominal skin, treating skin laxity in two directions. The umbilicus is handled along the same lines, transposed or reconstructed depending on its blood supply and position. See dual vector abdominoplasty.
 in Post Weight Loss Abdominoplasty (Tummy Tuck) 14")
Body lift (belt lipectomy). This removes a belt of skin right around the trunk. The umbilicus is transposed as part of the front portion of the operation. See body lift belt lipectomy after significant weight loss.
 in Post Weight Loss Abdominoplasty (Tummy Tuck) 15")
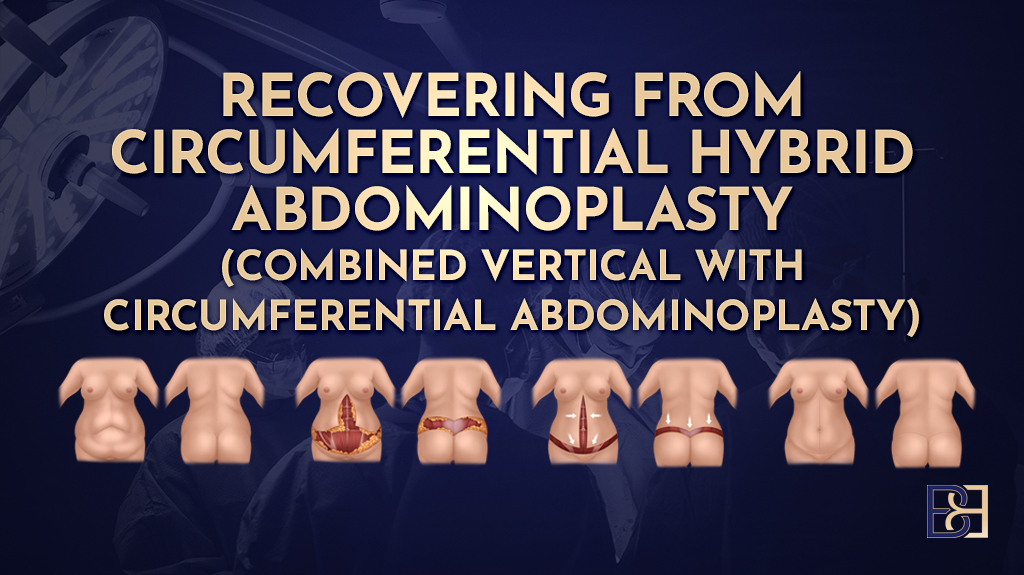
Circumferential hybrid abdominoplasty. This is a body lift with an added anterior vertical incision, combining the circumferential excision with a midline one at the front. The umbilicus is reconstructed within that anterior work. See circumferential hybrid abdominoplasty.
 in Post Weight Loss Abdominoplasty (Tummy Tuck) 16")
Apronectomy. This removes the overhanging apron of loose skin and fat from the lower abdomen, without lifting and advancing the upper skin the way a full abdominoplasty does. Because the upper skin is not advanced, the umbilicus is usually left in place rather than transposed. See apronectomy post weight loss.
 in Post Weight Loss Abdominoplasty (Tummy Tuck) 17")
Book your appointment online now
Standalone umbilicoplasty
Umbilicoplasty means reshaping the umbilicus itself. When performed on its own, without removing abdominal skin, it is a standalone umbilicoplasty.
This is a different situation from the one most of my post weight loss patients are in. Where there is loose abdominal skin to remove, the umbilicus is reconstructed as part of an abdominoplasty, as described above. A standalone umbilicoplasty suits a smaller number of people whose abdominal skin does not need contouring but who are bothered by the shape or position of the umbilicus or by a narrowing of its opening.
Can you have an umbilicoplasty without a tummy tuck (abdominoplasty)?
Yes. If the abdomen does not need skin removed, the umbilicus can be reshaped on its own. The decision rests on what the abdomen needs, which is assessed at consultation. For most post weight loss patients there is loose skin to treat, so umbilicoplasty forms part of the larger operation rather than a standalone one.
Is umbilicoplasty a major operation?
It is a smaller operation than an abdominoplasty, but it is still surgery and it still carries risk. Depending on the individual case, a standalone umbilicoplasty may be done under local anaesthetic, sometimes with sedation, and often as a day procedure. Whether that applies to you is decided at consultation, not in advance.
What happens during a standalone umbilicoplasty
The detail depends on what is being corrected. In general terms, I reshape the skin around the umbilicus, recess it where it protrudes, and where the opening has narrowed, a condition called umbilical stenosis, I release and reshape it. The umbilicus is then stitched into its new shape. The technique is matched to the individual umbilicus.
Will umbilicoplasty leave a scar?
Yes. All surgery leaves a scar. In umbilicoplasty, the incisions are placed within or around the rim of the umbilicus, so the resulting scar is kept as discreet as the anatomy allows. How a scar settles still varies from person to person, and I cover scarring in the risks section.
How long does umbilicoplasty last?
The result is usually long-term. Once it has healed, the reshaped umbilicus generally keeps its new shape. It can still change later with significant weight gain, weight loss, or pregnancy, because those are the forces that altered it in the first place. I cover that further on. Results vary between patients.
Umbilical hernia repair in the post weight loss patient
 in Post Weight Loss Abdominoplasty (Tummy Tuck) 18")
An umbilical hernia is where tissue pushes through a weak point in the abdominal wall at or near the umbilicus. The tissue may be fat, or in larger hernias a loop of bowel. It usually shows as a bulge at the belly button that can become more obvious when you cough, strain, or stand.
Umbilical hernias are common in patients who have carried significant weight. Raised abdominal pressure over time, a stretched and weakened abdominal wall, and previous pregnancies all make the area more prone to a hernia. For that reason I check for an umbilical hernia in every post weight loss patient I assess for abdominal surgery.
When is an umbilical hernia an emergency?
 in Post Weight Loss Abdominoplasty (Tummy Tuck) 19")
Most umbilical hernias are not an emergency. They become one when the tissue inside gets trapped and cannot be pushed back, called an incarcerated hernia, or when its blood supply is cut off, called a strangulated hernia. Warning signs include a hernia that becomes firm, painful, red or discoloured, will not go back in, or comes with nausea, vomiting, or fever.
A strangulated hernia is a surgical emergency. If you have these signs, do not wait for a routine appointment. Go to your nearest emergency department, or call 000 if you are very unwell.
Is it worth repairing an umbilical hernia?
That depends on the hernia and on you, and it is a clinical decision made at consultation rather than a fixed rule. A small hernia that causes no symptoms may reasonably be watched. A hernia that is enlarging, uncomfortable, or causing problems is usually worth repairing, both to settle the symptoms and to lower the chance of it becoming trapped. By “trapped,” I mean the tissue inside the hernia becoming stuck and losing its blood supply, which is the strangulated hernia emergency described above.
How long can a hernia be left untreated?
There is no single answer. A small, soft, painless hernia can often be monitored over time. What matters more than a set period is watching for change. If the hernia grows, becomes painful, or shows any of the emergency signs above, it needs to be assessed without delay.
Repairing a hernia at the same time as abdominoplasty
 in Post Weight Loss Abdominoplasty (Tummy Tuck) 20")
If you are having an abdominoplasty (tummy tuck) after weight loss and also have an umbilical hernia, I can usually repair the hernia during the same operation. Larger or recurrent hernias may need surgical mesh to reinforce the repair.
There is an important link between the two. The umbilicus draws its blood supply from the abdominal wall around its stalk, which is the same area a hernia repair works on. Repairing a hernia there can affect that blood supply. In some cases, I preserve and transpose the umbilicus as usual, and in others, it is the reason I construct a new umbilicus instead. I weigh this up during the operation.
How serious is umbilical hernia repair, and what is the recovery?
Umbilical hernia repair is a common operation, but it is still surgery, and it carries the general risks of surgery. Recovery varies between patients and depends on the size of the hernia, whether mesh was used, and whether it was repaired on its own or alongside an abdominoplasty.
On its own, a small umbilical hernia repair often allows a return to light activity within a couple of weeks, with heavier activity and lifting held off for longer on my advice. When the repair is part of an abdominoplasty, recovery follows the longer abdominoplasty timeline rather than the hernia one. I go through recovery in more detail below.+
Why is the umbilicus treated together with the abdomen?
For most post weight loss patients, a standalone umbilicoplasty is not the right option. The reason is straightforward. The umbilicus is stretched as part of the same loose skin that affects the whole abdomen. You cannot usually correct the stretched umbilicus on its own while leaving the loose abdominal skin around it untreated.
So in this group, the umbilicus is almost always reconstructed during an abdominoplasty (tummy tuck), as part of removing the loose abdominal skin. A standalone umbilicoplasty is reserved for the smaller number of people whose abdominal skin does not need contouring.
Who may be a candidate
 in Post Weight Loss Abdominoplasty (Tummy Tuck) 21")
There is no single profile that makes someone suitable for this surgery. Suitability is worked out for each person at consultation, after a GP referral. The factors below are the ones I weigh up.
- Stable weight. A result holds best when your weight has settled. Ongoing weight loss or regain can change the abdomen and the umbilicus again, so I prefer patients to be at a stable weight before surgery.
- General health. Surgery places demand on the body. I assess your medical history and any conditions, such as diabetes, that affect healing and anaesthetic risk.
- Not smoking. Smoking reduces the blood supply to the skin and raises the risk of wound problems and umbilical tissue loss. I ask patients to stop smoking for at least six weeks before and after surgery.
- Nutrition after weight loss. Many post weight loss patients have nutritional gaps that developed during weight loss, and these affect healing. Correcting them before surgery is part of preparing for it. I arrange blood tests during the lead-up, and you can read more in my guide to nutritional preparation before abdominoplasty.
- A clear understanding of what surgery involves. This covers the scars, the recovery, the risks, and the fact that results vary between patients. Surgery is one option, and it is not the right choice for everyone.
A GP referral is required before any consultation. Whether surgery is appropriate and which operation fits is decided at that consultation.
Timing
 in Post Weight Loss Abdominoplasty (Tummy Tuck) 22")
The main timing question after weight loss is whether your weight has settled.
- Wait until your weight is stable. I prefer your weight to have been steady for several months before surgery. If you have surgery while your weight is still changing, further loss or regain can alter the result, including the umbilicus.
- After bariatric surgery. Weight usually continues to decline for a time and then plateaus, often around 12 to 18 months after the operation. I generally wait until you have reached that plateau.
- After weight loss medications. The same principle applies, and your weight should be stable before surgery. If you are taking weight loss medications, we will discuss how they fit around your operation at the consultation. You should not adjust them on your own.
- Allow time to prepare. Nutritional preparation takes time, usually at least four weeks before surgery and longer where there is a deficiency to correct. This is built into the lead-up.
If your weight loss followed pregnancy, or you are also treating post pregnancy changes, I generally suggest waiting until you have finished having children and allowing around 12 months after a pregnancy for the body to settle. A later pregnancy can stretch the abdomen and umbilicus again and change the result.
Risks of umbilical reshaping
 in Post Weight Loss Abdominoplasty (Tummy Tuck) 23")
All surgery carries risk, and reshaping or reconstructing the umbilicus is no exception. The risks below are the ones specific to the umbilicus. When the umbilicus is reconstructed as part of an abdominoplasty (tummy tuck), the risks of that larger operation also apply, and I set those out in my guide to abdominoplasty risks and complications.
- Infection. Any wound can become infected. This may need antibiotics and, less often, a return to theatre.
- Reduced blood supply and tissue loss. The umbilicus depends on the blood supply through its stalk. If that supply is compromised, part or all of the umbilicus can lose viability, and the tissue can die, known as umbilical necrosis. This risk is higher in post weight loss patients, where the stalk is often long and thinned, and it is one reason I sometimes construct a new umbilicus rather than preserve the original.
- Umbilical stenosis. The opening can narrow as it heals, which can trap skin debris and may require a further procedure to release it.
- Scarring. Surgery always leaves a scar. Scars are permanent, and some people form thickened (hypertrophic) or raised (keloid) scars. How a scar settles varies from person to person.
- Asymmetry or an unintended shape or position. The healed umbilicus may not sit or look exactly as planned, and it can differ from side to side. A further procedure is sometimes needed to adjust it.
- Skin colour changes. Temporary redness is common as the area heals. Longer-lasting changes in skin colour around the umbilicus can also occur.
- Bleeding and bruising. Some bruising is expected. A collection of blood under the skin, called a haematoma, occasionally needs to be drained.
- Delayed healing or wound separation. The wound edges can be slow to heal or partially separate, particularly in smokers and in areas with reduced blood supply.
- Recurrence of the change. Significant weight gain, weight loss, or a later pregnancy can stretch the umbilicus again and undo the result.
- Blood clots. As with other surgeries, there is a risk of clots in the legs, called deep vein thrombosis, or in the lungs. This is more relevant when the umbilicus is reconstructed as part of a larger abdominoplasty. I assess and manage this risk for each patient, and I cover it in my article on DVT and body contouring surgery.
This is not a complete list. I go through the risks that apply to you and how I work to reduce them at the consultation. Results vary between patients.
Recovery
 in Post Weight Loss Abdominoplasty (Tummy Tuck) 24")
Recovery depends on which operation you have had. A standalone umbilicoplasty is a smaller operation with a shorter recovery. When the umbilicus is reconstructed as part of an abdominoplasty (tummy tuck), which is the usual situation after weight loss, recovery follows the longer timeline for abdominoplasty.
Recovery after a standalone umbilicoplasty
Expect some soreness, swelling, and bruising around the umbilicus for the first days to weeks. You will have dressing and wound care instructions, and I will ask you to keep the area clean and dry and to avoid straining and heavy lifting while it heals. Many people return to light activity within one to two weeks, though this varies. The early healing settles over the following weeks, and the scar continues to mature over months.
Recovery when the umbilicus is reconstructed during abdominoplasty
 in Post Weight Loss Abdominoplasty (Tummy Tuck) 25")
Here, the umbilicus is one part of a larger operation, so the recovery is the abdominoplasty recovery rather than a separate umbilical one. That involves a hospital stay, drains, a compression garment, and a staged return to activity and work over several weeks, with heavier activity and lifting held off for longer. Time off work depends on your job, with office-based work resuming sooner than manual work. I set this out in full in my guides to abdominoplasty recovery and to returning to work after abdominoplasty.
Either way, I review you in person at 4 weeks, 3 months, 6 months, and 12 months, and more often in the early weeks.
How painful is belly button surgery?
There is discomfort after any abdominal surgery, and the umbilicus is a sensitive area. Most of it is around the wound and is managed with pain relief that I prescribe and adjust. The discomfort settles as healing progresses, but pain thresholds and recovery vary from person to person, so I cannot tell you exactly how it will feel for you in advance.
How the scar settles over time
The scar is firmest and reddest in the early months, and softens and fades over the year or more that follows. I give you scar care advice at your reviews. How a scar finally settles still varies from person to person.
What about cost?
Cost depends on the operation, whether it is performed on its own or as part of an abdominoplasty, and the hospital and anaesthetic fees involved. Rather than quote a figure here, I provide a written, itemised quote with the full cost after consultation, and you can see current pricing on my price list. Some abdominoplasty procedures after weight loss may attract a Medicare item number when the criteria are met, and this is assessed individually.
Weight change or pregnancy after surgery
 in Post Weight Loss Abdominoplasty (Tummy Tuck) 26")
The umbilicus was changed in the first place by weight gain, weight loss, and in some patients, pregnancy. Those same forces can change it again after surgery.
Significant weight regain or further weight loss can stretch and distort the abdomen and umbilicus once more. This is why I encourage maintaining a stable weight both before and after surgery, so the result is more likely to hold.
A pregnancy after surgery stretches the abdomen and the umbilicus as it grows. There is nothing wrong with becoming pregnant after an umbilicoplasty or an abdominoplasty, but it can stretch the area again and alter the result, and a further procedure may be wanted later. If you are planning more children, it is worth raising at the consultation so we can factor it into timing.
What this means for you
 in Post Weight Loss Abdominoplasty (Tummy Tuck) 27")
In post weight loss patients, the umbilicus is rarely treated on its own. It is stretched as part of the same loose skin that affects the abdomen, so in most cases, it is reconstructed during an abdominoplasty (tummy tuck), using the approach that fits the operation and the condition of the umbilicus itself. A standalone umbilicoplasty has its place, but for fewer people in this group.
Whether any of this is right for you, and which approach to take, is a clinical decision made with you at consultation, after a GP referral. Surgery is one option among others; it carries real risks, and results vary from patient to patient.
References
- Graham KA, Livingston RJ. Ideal male umbilicus: an observational study of surface anatomy and introduction to the SHAPE classification. Aesthetic Plast Surg. 2022;46(5):2333-2341.
- Ngaage LM, Kokosis G, Kachniarz B, Pedreira R, Rada EM, Nam AJ, et al. A two-step technique for neo-umbilicoplasty in the abdominal reconstructive population. Plast Reconstr Surg Glob Open. 2019;7(7):e2341.