Losing a large amount of weight is a major achievement, whether you reached your goal through diet and exercise, weight loss medications, or bariatric surgery. For many of the people I see in my practice, that achievement comes with a frustrating physical reality. Once the weight is gone, the skin that stretched to accommodate it often does not shrink back. You are left with loose, hanging skin across the abdomen that no amount of further dieting or training will tighten.
An abdominoplasty (tummy tuck) removes this excess skin and reshapes the abdomen once your weight has settled. Body contouring surgery for people who have had significant weight loss makes up a large part of my work, and this guide reflects what I see and do for these patients.
 After Weight Loss: A Complete Guide for Post Weight Loss Patients 1")
 After Weight Loss: A Complete Guide for Post Weight Loss Patients 2")
Why a guide written for post weight loss patients
Most general information about tummy tuck (abdominoplasty) surgery is written with the post-pregnancy patient in mind. The post weight loss abdomen is different, and the surgery has to account for that.
After pregnancy, the main problem is often separated abdominal muscles (diastasis recti) with a relatively modest amount of loose skin. After major weight loss, the picture is usually the reverse. There is a large volume of loose skin, the laxity frequently extends around the flanks and lower back, and the belly button (umbilicus) is commonly stretched and pulled downward rather than deeply set. Many post weight loss patients do not have significant muscle separation (diastasis recti) at all. Planning the operation around the post-pregnancy model misses what these patients actually need.
This guide reflects what I see and do for post weight loss patients specifically.
What this guide covers
The Post Weight Loss Abdomen and How It Presents
When a post weight loss patient comes to see me, the weight has usually already gone. The problem that remains is the skin. Understanding how the abdomen presents after major weight loss explains why the surgery is planned the way it is.
Loose, overhanging skin
 After Weight Loss: A Complete Guide for Post Weight Loss Patients 3")
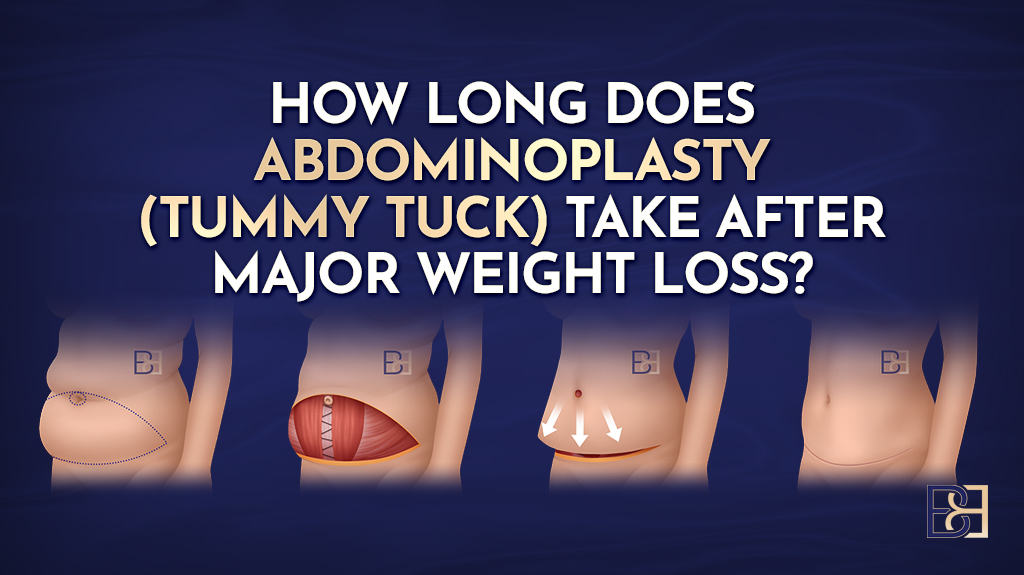
The most common finding is a large amount of loose skin across the lower abdomen, often hanging as an apron over the pubic area and upper thighs. Skin has a limited ability to shrink back after it has been stretched for a long time. When weight is lost slowly or through rapid weight loss, and especially after massive weight loss, skin elasticity is reduced and the skin does not retract to fit the smaller frame underneath.
This is not something further weight loss, creams, or exercise can fix. Once the skin has lost its elastic recoil, surgery to remove the excess is the only reliable way to deal with it.
The belly button (umbilicus)
In post weight loss patients the belly button (umbilicus) is usually stretched and pulled downward, sitting lower than it should and elongated by the weight of the overhanging skin. This is different from the deeply set, funnelled belly button often seen after pregnancy. It is one of the reasons a standard post-pregnancy approach does not translate directly to these patients, and it shapes how the umbilicus is handled during surgery.
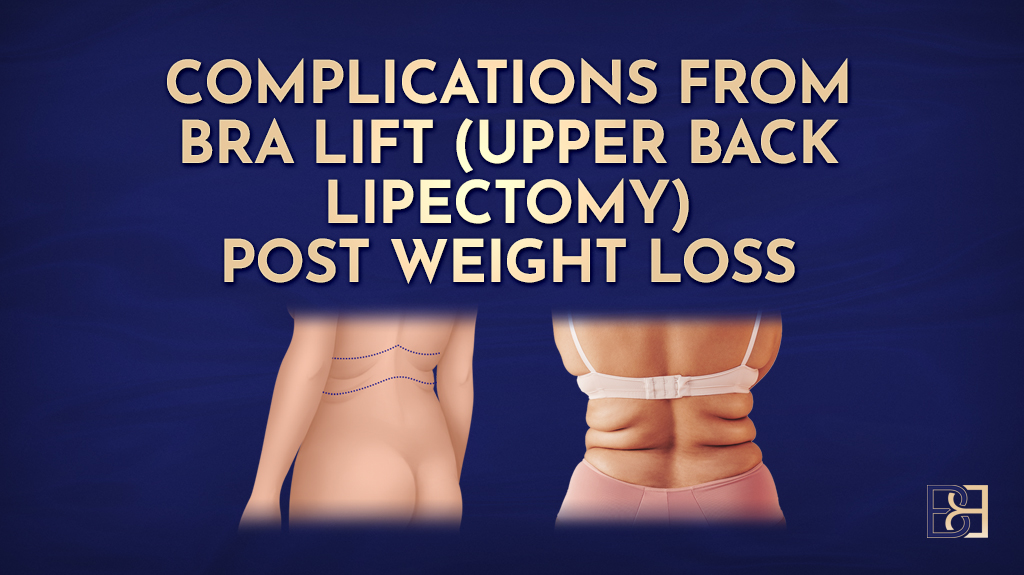
Where the laxity extends
Loose skin after major weight loss rarely stays neatly on the front of the abdomen. It commonly continues around the flanks and into the lower back, and the mons pubis is frequently involved as well. The pattern is often closer to a circumferential one than a front-of-abdomen problem alone. Assessing how far the laxity extends is a key part of working out which operation fits.
Muscle separation (diastasis recti) is not the usual driver
 After Weight Loss: A Complete Guide for Post Weight Loss Patients 4")
Separated abdominal muscles (diastasis recti) are mainly a post-pregnancy problem, caused by the abdominal wall stretching to accommodate a growing baby. Many post weight loss patients do not have significant abdominal muscle separation (diastasis recti) at all. Some do, particularly those who have also been through pregnancy, and where it is present it can be repaired during the operation. The point is that muscle repair is not assumed for these patients the way it often is after pregnancy. Whether the abdominal wall needs anything done to it is assessed for each person individually.
Day to day effects of the excess skin
 After Weight Loss: A Complete Guide for Post Weight Loss Patients 5")
Beyond appearance, the overhanging skin can cause practical problems. Patients often describe:
- Skin irritation, rashes, and recurrent infection where skin folds rub and trap moisture (intertrigo)
- Difficulty with hygiene in the skin folds
- Trouble finding clothing that fits
- Restriction with exercise and movement
These functional issues are a common reason post-weight loss patients look into surgery, not just the look of the abdomen.
Am I a Candidate for Abdominoplasty After Weight Loss?
Not everyone who has lost weight is ready for surgery straight away. Whether an abdominoplasty (tummy tuck) is the right step depends on a few things I work through with each patient.
Stable weight
 After Weight Loss: A Complete Guide for Post Weight Loss Patients 6")
The single most important factor is a stable weight. I want patients to be at or near the weight they intend to maintain, and to have held that weight steady for around six to twelve months before surgery.
This matters on both sides. If you are still actively losing weight, more loose skin will develop after the operation, which can compromise the result. If your weight is still fluctuating, the outcome is harder to predict. Surgery works best once the weight loss is complete and settled.
An abdominoplasty (tummy tuck) is not a weight loss operation. It removes loose skin and excess tissue. It is not a substitute for reaching your goal weight first.
General health and fitness
Body contouring surgery after major weight loss is a substantial operation, and a longer operation places more demand on the body. I assess your overall health, fitness, and any medical conditions to work out whether you are well enough to recover well.
 After Weight Loss: A Complete Guide for Post Weight Loss Patients 7")
Smoking matters here. Smoking reduces blood supply to healing tissue and raises the risk of wound healing problems. I ask patients to stop well before surgery.
Nutritional readiness
 After Weight Loss: A Complete Guide for Post Weight Loss Patients 8")
Most post weight loss patients have some nutritional gaps that developed during weight loss, particularly after weight loss surgery (bariatric surgery). Low iron, vitamin D, B12, and protein stores are common, and they all matter for wound healing. Correcting these before surgery is part of preparing properly.
Every post weight loss patient I operate on has a standard pre-operative blood panel to check for these gaps, and I work with the patient, their GP, and a dietitian to put anything right beforehand. I cover this in detail in my nutrition articles on protein, nutritional deficiencies after bariatric surgery, and preparing for abdominoplasty (tummy tuck) surgery after weight loss.
BMI as a guide, not a cut-off
 After Weight Loss: A Complete Guide for Post Weight Loss Patients 9")
Body mass index (BMI) is a rough guide only. I do not use a hard BMI cut-off, because it does not tell the whole story. Two people with the same BMI can carry their weight very differently and have very different amounts of loose skin. Clinical assessment of your individual situation matters more than a single number. Routine DEXA scans are not part of how I assess candidacy.
Realistic expectations
It helps to be clear about what the surgery does and does not do. An abdominoplasty (tummy tuck) removes loose abdominal skin and excess tissue and reshapes the area. It leaves permanent scars, which I place where they can be covered by underwear or swimwear where possible. It does not remove every contour irregularity, it does not stop future weight change, and it is not a treatment for stretch marks beyond the skin that is removed.
Thinking about future pregnancy
 After Weight Loss: A Complete Guide for Post Weight Loss Patients 10")
If you are considering future pregnancies, it is important to discuss this during your consultation. Pregnancy after an abdominoplasty (tummy tuck) can stretch the repaired tissue again and affect the result, so timing is something to talk through before deciding when to operate.
The Procedure Types I Use After Weight Loss
There is no single tummy tuck (abdominoplasty). The right operation depends on how much loose skin you have and where it sits. Some patients have an overhang limited to the lower abdomen. Others have laxity that runs around the flanks and back, or excess in both the up-and-down and side-to-side directions. Below are the main approaches I use, from less to more extensive. Which one fits is worked out at consultation, and the decision is covered in more detail in the section on single versus staged surgery.
Apronectomy
 After Weight Loss: A Complete Guide for Post Weight Loss Patients 11")
An apronectomy removes the overhanging apron of loose lower abdominal skin, sometimes called a pannus. It is a lower-burden operation. It does not reposition the belly button (umbilicus), tighten the upper abdomen, or do anything to the abdominal wall. It removes the excess skin at the front.
This suits patients whose main problem is a lower abdominal overhang, and patients for whom a longer, more involved operation is not appropriate. For post weight loss patients, an apronectomy is far more relevant than a limited abdominoplasty. A limited abdominoplasty treats only a small amount of lower skin laxity and rarely fits the post weight loss abdomen.
I cover this further in my article on apronectomy after weight loss.
Full abdominoplasty (tummy tuck)
 After Weight Loss: A Complete Guide for Post Weight Loss Patients 12")
A full abdominoplasty, also called a full tummy tuck, removes excess skin from the lower abdomen, tightens the skin from the rib margin down to the pubic area, and repositions the belly button (umbilicus). The incision runs low across the abdomen from hip to hip, placed so it can sit below underwear or swimwear. If muscle separation (diastasis recti) is present it can be repaired at the same time, though as noted earlier many post weight loss patients do not need this.
Fleur-de-Lis abdominoplasty
 After Weight Loss: A Complete Guide for Post Weight Loss Patients 13")
When a patient has a large amount of loose skin in the side-to-side direction as well as up and down, a standard horizontal removal alone will not deal with it. A Fleur-de-Lis abdominoplasty adds a vertical incision down the midline of the abdomen, which lets me remove width as well as length. The result is a scar in both directions, horizontal across the lower abdomen and vertical up the midline.
This is common in post weight loss patients, who often carry significant horizontal skin excess. I cover the technique in detail in my article on Fleur-de-Lis abdominoplasty after weight loss.
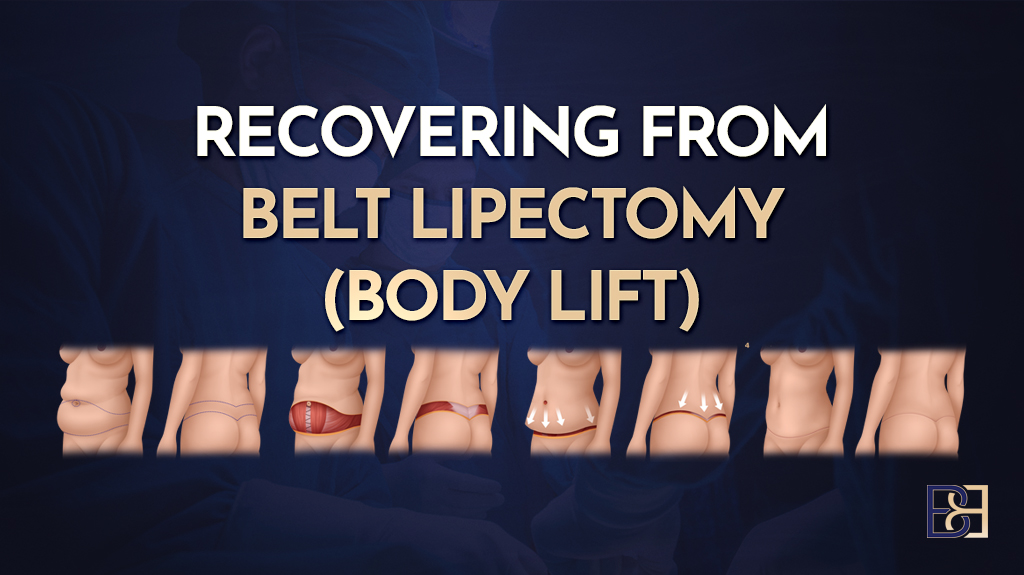
Body lift (belt lipectomy)
 After Weight Loss: A Complete Guide for Post Weight Loss Patients 14")
When the loose skin continues around the flanks, lower back, and buttocks rather than staying at the front, the laxity is circumferential and needs to be treated all the way around. A body lift (belt lipectomy) removes a belt of skin around the entire trunk, mainly the vertical, up-and-down excess. The same operation is also called a circumferential abdominoplasty, a circumferential body lift (belt lipectomy), or a 360-degree body lift (belt lipectomy). The back portion of the operation, the back lipectomy, lifts the buttock and the outer thigh at the same time. The scar runs around the body, again placed low where it can be covered.
I cover this further in my article on body lift (belt lipectomy) after weight loss.
Dual vector abdominoplasty
 After Weight Loss: A Complete Guide for Post Weight Loss Patients 15")
A dual vector abdominoplasty is an approach I use for patients who have significant laxity in both vertical planes, the lower and the upper abdomen. It combines a Fleur-de-Lis with removal of upper abdominal skin, treating excess that a standard approach would leave behind. It is suited to a particular pattern of laxity rather than being a step up or down from the Fleur-de-Lis.
Circumferential hybrid abdominoplasty
 After Weight Loss: A Complete Guide for Post Weight Loss Patients 16")
A body lift (belt lipectomy) mainly removes the vertical, up-and-down excess around the trunk. When a patient also has significant side-to-side, horizontal excess across the front of the abdomen, that width is left behind. A circumferential hybrid abdominoplasty is an approach I use in this situation. It combines a body lift (belt lipectomy) with an anterior vertical incision that removes the horizontal excess on the front of the abdomen, which makes it a more complete treatment for loose lower trunk skin. As with a body lift (belt lipectomy), the back portion lifts the buttock and outer thigh.
Combined suction-assisted lipectomy (liposuction)
 After Weight Loss: A Complete Guide for Post Weight Loss Patients 17")
In some patients I use suction-assisted lipectomy (liposuction) alongside skin removal to refine the contour of the flanks or upper abdomen. Liposuction removes fat, not loose skin, so it is an adjunct to the skin-removing operation rather than a treatment for laxity on its own.
Single Comprehensive Operation Versus Staged Surgery
A common question is whether the work can be done in one operation or whether it needs to be split into stages. There is no single answer that fits everyone.
My preference, where a patient is suited to it
Where a patient is medically suited to it, I prefer to treat their loose skin in one comprehensive operation rather than dividing it across several separate procedures. The reasoning is practical. One operation means one anaesthetic, one hospital admission, and one recovery period to work through, rather than repeating each of those steps two or three times.
This is a preference, not a rule, and it is never a reason to expand the scope of someone’s surgery beyond what they need.
The trade-off
 After Weight Loss: A Complete Guide for Post Weight Loss Patients 18")
A larger single operation is a bigger physiological event than a smaller one. A longer operating time places greater demand on the body, and recovery from a comprehensive operation should not be underestimated. This is the trade-off, and it is the reason pre-operative preparation matters more when a single comprehensive operation is planned, not less.
When staging is the better path
For some patients, doing everything at once carries more physiological demand than is sensible. In that situation, staging the work across separate operations is the more appropriate and considered path. This can be the case when medical factors require the work to be spread out, or when the extent of the loose skin cannot be treated well in a single operating time.
Staging is a legitimate clinical choice. It is the right approach for some patients, and it is not a lesser option or a compromise.
How the decision is made
 After Weight Loss: A Complete Guide for Post Weight Loss Patients 19")
Whether one operation or staged surgery suits you is a clinical judgement I make with each patient. It follows assessment of your medical history, your nutritional status, the pattern and extent of your loose skin, and what can be done well in a single operating time. It is worked through together, based on what is appropriate for you as an individual, rather than decided in advance.
Why this connects to preparation
Because a larger single operation is a more demanding event, getting the preparation right carries more weight. Most post weight loss patients have nutritional gaps that developed during weight loss, and correcting those beforehand supports healing. When a comprehensive operation is planned, that preparation is part of making the larger operation an appropriate choice in the first place.
Weight Stability and the Effect of Weight Regain
 After Weight Loss: A Complete Guide for Post Weight Loss Patients 20")
The result of an abdominoplasty (tummy tuck) is closely tied to your weight, both before and after surgery. This is worth understanding before you decide on timing.
Why the result is calibrated to your weight at the time of surgery
When I operate, the amount of skin I remove is matched to your frame at that point. The closer you are to a settled, maintainable weight, the more predictable the outcome.
If you go on to lose a significant amount more weight after surgery, the skin that is left can become loose again, because there is now less underneath it. If you gain a significant amount, the skin stretches to accommodate it. Either way, large weight changes after surgery can work against the result.
What weight regain does
Significant weight regain after an abdominoplasty (tummy tuck) can stretch the skin and soft tissue again and undo part of the improvement. It can also widen or thicken the scar over time. This is why I ask patients to be at a weight they can realistically hold before we operate.
Small fluctuations of a few kilograms are normal and not a problem. The concern is large or repeated swings in body weight, sometimes called significant weight fluctuations, which make the long-term outcome harder to hold.
Maintaining your result
 After Weight Loss: A Complete Guide for Post Weight Loss Patients 21")
An abdominoplasty (tummy tuck) removes loose skin. It does not change your weight by much, and it does not prevent future weight gain. Holding onto the result over the years comes down to the same things that helped you lose the weight in the first place: a balanced diet, regular activity, and a healthy lifestyle. The surgery deals with the skin that will not retract. Keeping a steady weight afterwards is what protects the outcome and your body shape.
Results vary
Results vary between patients. How an individual heals and how the contour settles depends on several factors, including skin quality, the extent of the loose skin, your weight stability, your nutritional status, and your general health. No two patients are the same, and the result for any one person cannot be promised in advance.
Preparing for Surgery
 After Weight Loss: A Complete Guide for Post Weight Loss Patients 22")
Good preparation is a large part of a good recovery, and it matters more after major weight loss, not less. A comprehensive operation places real demand on the body, so the work done in the weeks and months beforehand counts.
Nutritional optimisation
 After Weight Loss: A Complete Guide for Post Weight Loss Patients 23")
Most post weight loss patients have nutritional gaps that developed while they were losing weight, and these are more pronounced in post bariatric patients. Low iron, vitamin D, B12, folate, and protein stores are common, and each of these affects wound healing, with gaps raising the risk of poor wound healing. Correcting them before surgery gives the body what it needs to repair afterwards.
Supplementation follows a tiered approach. There is a core set I use for all post weight loss patients (Tier 1), and a second set guided by what your own blood results show (Tier 2). I do not set out the full protocol here, because the blood-guided part depends on your individual results. The detail is in my nutrition articles, including protein after weight loss, nutritional deficiencies after bariatric surgery, and the vitamins and supplements hub. The on-ward dietitian at Maitland Private Hospital is available to review your nutrition if any issues arise around the time of surgery, and your GP looks after the longer term.
The pre-operative blood panel
 After Weight Loss: A Complete Guide for Post Weight Loss Patients 24")
Every post weight loss body contouring patient I operate on has a comprehensive pre-operative blood panel. It checks full blood count, clotting, liver and kidney function, glucose and HbA1c, thyroid function, iron studies, and a range of vitamins and minerals including vitamin D, B12, folate, vitamin A, vitamin E, zinc, and selenium. Albumin is used as the marker of protein status. Your GP is copied in on these results so the whole team is working from the same information. I go through what each test means in my article on the pre-operative blood panel.
Weight loss medications around surgery
 After Weight Loss: A Complete Guide for Post Weight Loss Patients 25")
Many of my patients have used weight loss medications. Current Australian perioperative guidance does not recommend routinely stopping these medications before surgery, and I follow that position (1). In some cases, where protein intake targets are difficult to meet, a temporary dose adjustment may be discussed as part of perioperative planning. This is a decision made with you and your treating team. It is not something to adjust on your own.
Medication review and blood thinners
I review all your medications before surgery. Blood-thinning medications such as aspirin and anticoagulants are usually stopped about a week before the operation, planned well in advance. Some patients need to continue them through surgery, which is also planned ahead of time. Either way, these medications should never be stopped or changed without instruction.
Anaesthetic assessment
 After Weight Loss: A Complete Guide for Post Weight Loss Patients 26")
For most patients the anaesthetic consultation happens by phone. The physical examination, including assessment of your airway, is done on the day of surgery. An in-person anaesthetic review before the day of surgery is uncommon.
What Happens During the Operation
 After Weight Loss: A Complete Guide for Post Weight Loss Patients 27")
Book your appointment online now
This is a general outline of how the operation runs. The exact steps depend on which procedure you are having, but the principles below apply across the post weight loss abdominoplasty (tummy tuck) operations I perform.
Anaesthetic
The operation is done under a general anaesthetic. The anaesthetic assessment is covered in the preparation section above.
The incision
 After Weight Loss: A Complete Guide for Post Weight Loss Patients 28")
For a standard abdominoplasty (tummy tuck) the main incision runs low across the abdomen in a hip to hip incision, placed so it sits below underwear or swimwear where possible. A Fleur-de-Lis abdominoplasty adds a vertical incision up the midline. A body lift (belt lipectomy) continues the incision around the trunk. Where the incision goes is planned and marked before surgery, with you standing, so the skin is removed in the right amount and the right direction.
Lifting the skin and the plane I work in
Once the incision is made, I lift the loose skin and fat off the abdominal wall. I keep the dissection in the plane just deep to Scarpa’s fascia, a strong layer within the fatty tissue. This keeps Scarpa’s fascia inside the skin flap and leaves the deeper fat and the lymphatic channels undisturbed on the abdominal wall. Preserving those lymphatics helps reduce fluid build-up after surgery and supports healing (2).
The belly button (umbilicus)
 After Weight Loss: A Complete Guide for Post Weight Loss Patients 29")
In post weight loss patients the belly button (umbilicus) is usually stretched and sitting low. The stalk is freed from the surrounding skin, then trimmed and shortened at its base with sutures to treat the stretching. It is then brought out through a new, correctly positioned opening once the loose skin has been removed. I describe this in more detail in my article on reconstructing the belly button (umbilicus) in post weight loss abdominoplasty.
Muscle repair, if needed
 After Weight Loss: A Complete Guide for Post Weight Loss Patients 30")
If muscle separation (diastasis recti) is present, the abdominal wall is tightened with sutures at this stage. As covered earlier, many post weight loss patients do not have significant separation and do not need this step.
Removing the excess skin and closing
The excess skin and tissue are removed, and the layers are closed carefully. I repair Scarpa’s fascia as part of the closure, which takes tension off the skin and supports the scar through the healing process.
Drains
 After Weight Loss: A Complete Guide for Post Weight Loss Patients 31")
I place two closed suction drains, one on each side, exiting near the lateral hip. They draw off the fluid that collects after surgery. The drains stay in until the output drops below a set level, usually somewhere between two and seven days. I use a drainless technique for some post pregnancy abdominoplasty (tummy tuck) patients. In post weight loss patients the amount of skin removed is much larger, which leaves a bigger space where fluid can collect, so I do not usually use a drainless approach in this group. Drains are the better choice here.
Dressings and compression garment
 After Weight Loss: A Complete Guide for Post Weight Loss Patients 32")
The wounds are covered with PICO negative pressure dressings. These are changed at around day seven to a Hypafix tape dressing. A compression garment is fitted, and how it is worn afterwards is covered in the recovery section.
Recovery After Abdominoplasty (Tummy Tuck) Following Weight Loss
Recovery is a process that runs over weeks and months, not days. Here is what to expect through the stages, keeping in mind that a comprehensive operation after weight loss is major surgery and a larger event that should be given time.
In hospital
Most patients stay two to four nights. On the first day after surgery I want you out of bed and walking. If your blood pressure makes standing difficult to begin with, sitting out of bed is the first step, and we build from there. Getting moving early is one of the most useful things you can do. It helps your recovery and lowers the risk of blood clots. Pain is managed with medication during your stay.
Drains and dressings
 After Weight Loss: A Complete Guide for Post Weight Loss Patients 33")
The drains placed during surgery stay in until the fluid output drops below a set level, usually between two and seven days. The PICO dressings are changed at around day seven to a Hypafix tape dressing, which is simpler to manage at home.
The compression garment
You will wear a compression garment full-time for the first four weeks, then half-time for a further two weeks. I prefer daytime wear, because swelling tends to be worse throughout the day. There is room for flexibility, such as wearing it overnight in hot weather or to suit your own comfort. The garment helps reduce swelling and supports the healing tissues.
Pain and discomfort
 After Weight Loss: A Complete Guide for Post Weight Loss Patients 34")
Expect physical discomfort, tightness, and a pulling sensation across the abdomen in the first couple of weeks, particularly when you stand up straight or move. This is normal and is managed with pain medication. It settles steadily over the following weeks.
Swelling, numbness, and the scar
Swelling builds in the first week or so and then settles gradually over the following months. Numbness or altered skin sensation in the lower abdomen is common, because small sensory nerves are interrupted during surgery. Sensation usually returns over several months, though some areas can stay slightly numb. The scar is firm and pink at first, then softens and fades over twelve months or more.
Getting back to activity
 After Weight Loss: A Complete Guide for Post Weight Loss Patients 35")
Start with light walking and build up gradually. Avoid strenuous exercise and heavy lifting in the early weeks. Because many post weight loss patients do not have muscle separation (diastasis recti), they can often return to core exercises and squats from around four weeks, which is earlier than someone who has had a muscle repair. I set out activity timelines in detail in my article on exercise after abdominoplasty (tummy tuck) following weight loss.
Returning to work
 After Weight Loss: A Complete Guide for Post Weight Loss Patients 36")
If your work is sedentary, plan for around four weeks off. If your work involves manual or physical labour, plan for six to eight weeks. Clearance to return is given at whichever post-operative visit you are ready, not only at the four-week mark. I cover this in my article on returning to work after abdominoplasty (tummy tuck) following weight loss.
Follow-up
 After Weight Loss: A Complete Guide for Post Weight Loss Patients 37")
I review you at four weeks, three months, six months, and twelve months after surgery. At the four-week visit I hand over to your GP for ongoing care, passing on your blood results, the operation details, and your supplement records so your long-term management stays joined up.
Warning signs and who to contact
 After Weight Loss: A Complete Guide for Post Weight Loss Patients 38")
After hours, your first call is to Maitland Private Hospital, where a nurse will triage your concern by phone. Anything that needs a physical assessment is directed to your local emergency department. For anything life-threatening, call 000. Maitland Private Hospital is not an emergency department. Contact someone promptly if you have unusual or severe pain, increasing redness or discharge from the wound, a fever, or calf pain, swelling, or breathlessness.
Risks and Complications
Every operation carries risks, and a larger operation after weight loss carries more of them than a smaller one. You should understand these before you decide. Post weight loss patients also have somewhat higher rates of certain complications, particularly with wound healing, because the wounds are larger and major weight loss changes the body’s nutritional reserves (3). Preparing well reduces these risks but does not remove them.
Bleeding and haematoma
 After Weight Loss: A Complete Guide for Post Weight Loss Patients 39")
Some bleeding is normal. Occasionally, blood collects under the skin (a haematoma) and needs to be drained, sometimes in a return to theatre. Stopping blood-thinning medications as planned before surgery reduces this risk.
Seroma
A seroma is a collection of fluid under the skin flap. It is one of the more common issues after this surgery, and post weight loss patients are more prone to it because removing a large amount of skin leaves a bigger space where fluid can gather. This is the reason I use drains rather than a drainless approach in these patients. A seroma that persists may need to be drained with a needle in clinic.
Infection
 After Weight Loss: A Complete Guide for Post Weight Loss Patients 40")
Any surgical site can become infected. Signs include increasing redness, warmth, pain, or discharge. Most wound infections are treated with antibiotics, though a more significant one occasionally needs further treatment.
Wound healing problems
Healing can be slow, and the wound can separate in places, most often where the incisions meet, such as the junction of the vertical and horizontal scars in a Fleur-de-Lis abdominoplasty. Smoking, diabetes, and poor nutrition all raise this risk, which is why I work on these things before surgery. Slow-healing wounds are managed with dressings and time.
Skin and fat necrosis
When a large skin flap is lifted, its blood supply can occasionally be reduced at the edges, and a small area of skin or fat can break down. This is more likely in smokers. It is managed with wound care and, in some cases, a minor further procedure.
Blood clots (deep vein thrombosis)
 After Weight Loss: A Complete Guide for Post Weight Loss Patients 41")
A clot in the leg veins (deep vein thrombosis) can form after surgery, and rarely a clot can travel to the lungs, which is serious. Longer operations and the post weight loss patient group both carry a higher risk. I assess your individual clot risk and decide on the appropriate preventive measures myself, rather than leaving it to the anaesthetist. These measures, along with getting you moving early, are aimed at lowering the risk. I cover this fully in my article on deep vein thrombosis risk and prevention after body contouring surgery.
Scarring and scar revision
 After Weight Loss: A Complete Guide for Post Weight Loss Patients 42")
The scars are permanent. They are placed low and where clothing can cover them, but they can sometimes widen or thicken, and occasionally a scar revision is worth considering down the track. I discuss scar management in my article on scars and scar revision after abdominoplasty (tummy tuck).
Altered sensation
As covered in the recovery section, numbness or changed sensation around the lower abdomen is common after surgery and usually improves over months, though some areas can stay slightly numb.
Asymmetry, contour irregularity, and revision surgery
The two sides may not settle exactly evenly, and minor contour irregularities or small areas of extra skin at the ends of the incision can occur. Some patients choose a small revision procedure later to refine the result.
Anaesthetic risks
A general anaesthetic carries its own risks. These are uncommon in a well-prepared patient and are something your anaesthetist will go through with you.
Before you decide on surgery, I go through the risks that apply to your particular situation, given your health, the procedure planned, and whether the work is done in one operation or staged.
Cost
 After Weight Loss: A Complete Guide for Post Weight Loss Patients 43")
The cost of surgery depends on which operation you have, how complex it is, the length of the operation, the anaesthetic, and your hospital stay. Because these vary from patient to patient, I do not quote a single price here. After your consultation you receive an itemised quote that sets out exactly what is included, and a pricelist is available.
Medicare and private health insurance
Some post weight loss patients meet the criteria for a Medicare item number. This applies where the surgery is assessed as reconstructive surgery rather than cosmetic surgery, for example where a significant skin overhang is causing documented problems such as recurrent skin infection. Where a Medicare item number applies, a private health insurance rebate may also be available, depending on your level of cover. Eligibility is assessed against the specific Medicare criteria for each patient and cannot be assumed in advance. Your itemised quote reflects whether an item number applies to your situation.
Frequently Asked Questions
How long should I wait after losing weight before having surgery?
I want you at or near a weight you can maintain, and holding it steady for around six to twelve months. Operating before your weight has settled makes the result less predictable.
Is an abdominoplasty (tummy tuck) a way to lose weight?
No. It removes loose skin and excess tissue that will not retract after weight loss. It does not change your weight by much and is not a substitute for reaching your goal weight first.
Can I have surgery if I lost the weight through bariatric surgery?
Yes. Many of my post weight loss patients have had bariatric surgery. The main things to sort out first are a stable weight and any nutritional gaps, which is why the pre-operative blood panel matters.
Will I definitely need muscle repair?
Not necessarily. Muscle separation (diastasis recti) is mainly a post-pregnancy issue. Many post weight loss patients do not have it, so muscle repair is not assumed and is only done if you need it.
Will I have drains?
Yes. For post weight loss patients I use two closed suction drains, because the larger amount of skin removed leaves more space for fluid to collect. They usually come out within two to seven days.
How visible will the scars be?
The scars are permanent. I place the main scar low so it can sit under underwear or swimwear. A Fleur-de-Lis abdominoplasty also leaves a vertical scar up the midline, and a body lift (belt lipectomy) leaves a scar that continues around the trunk.
When can I go back to work?
Around four weeks for sedentary work, and six to eight weeks for manual or physical work. I give clearance at whichever follow-up visit you are ready.
Can I get pregnant after an abdominoplasty (tummy tuck)?
Yes, but a pregnancy can stretch the tissue again and affect the result. If you are planning a pregnancy, it is worth raising at consultation so we can think about timing.
Will Medicare or my health fund cover it?
Some post weight loss patients meet the criteria for a Medicare item number, which can also open up a private health insurance rebate. Eligibility depends on meeting specific criteria and is assessed for each patient.
References
- Hocking SL, Scott DA, Remedios ML, Horowitz M, Story DA, Greenfield JR, et al. 2025 ADS/ANZCA/GESA/NACOS clinical practice recommendations on the peri-procedural use of GLP-1/GIP receptor agonists. Anaesth Intensive Care. 2025;53(5):300-306.
- Costa-Ferreira A, Rebelo M, Silva A, Vásconez LO, Amarante J. Scarpa fascia preservation during abdominoplasty: randomized clinical study of efficacy and safety. Plast Reconstr Surg. 2013;131(3):644-651.
- Makarawung DJS, Al Nawas M, Smelt HJM, Monpellier VM, Wehmeijer LM, van den Berg WB, et al. Complications in post-bariatric body contouring surgery using a practical treatment regime to optimise the nutritional state. JPRAS Open. 2022;34:91-102.