Loose skin after weight loss does not present in one single way. For some patients, it is mainly a hanging fold low on the abdomen. For others, the looseness runs horizontally across the front, vertically along the midline, or in a circumferential pattern around the trunk. Loose skin in the lower chest, back, and thighs is often part of the picture as well. After massive weight loss, the skin has usually lost much of its elasticity, often leaving stretch marks, and the change in body shape can be considerable.
 Do I Need After Weight Loss? Matching the Operation to Your Skin Pattern 1")
 Do I Need After Weight Loss? Matching the Operation to Your Skin Pattern 2")
That variety is what makes planning so different for post-weight-loss patients. There is always a compromise between how much skin can be removed, how many incisions are made, and how much scarring that takes. Many of my post-weight-loss patients want to remove as much loose skin as possible in a single operation, and there are several ways to approach that. Which one suits you depends on the pattern of your loose skin, your general health, and your nutritional status. Two patients who have lost a similar amount of weight can still need quite different operations because their skin has settled differently.
Why the Usual “Types of Abdominoplasty (Tummy Tuck)” Operations Don’t Apply to Weight Loss Patients
Most articles on this topic are written for women after pregnancy. They lead with a muscle separation (diastasis recti) and a full abdominoplasty (tummy tuck), using a hip-to-hip incision with muscle repair to treat the separated abdominal muscles.
Post-weight-loss patients are usually in a different position:
- The loose skin is more extensive, and it often does not stop at the front of the abdomen. It can continue around the hips and back.
- Many post weight loss patients do not have significant muscle separation (diastasis recti), so muscle repair is not always part of the plan. When pregnancy is also part of the picture, I assess it individually.
- A limited abdominoplasty (mini abdominoplasty) is essentially a post-pregnancy operation. It is not something I use after major weight loss because it does not treat enough skin.
So the question is less “which type of abdominoplasty (tummy tuck) is best” and more “where is your loose skin, and what will it take to treat it well in one operation?”
What this article covers
I will walk through how I match the operation to your skin pattern, the operations I use most often after weight loss, and the choice between doing the work in a single, larger operation or staging it across multiple operations. I will also cover what I assess at consultation, how preparation before surgery matters, and the recovery and risks you should weigh up.
Why is the decision different after weight loss?
When someone comes to see me after major weight loss, the assessment differs from that of a post-pregnancy consultation. A few things drive that.
Loose skin pattern leads, not muscle repair
After significant weight loss, the main problem is excess skin. The fat has gone, but the skin that stretched to cover it does not shrink back. That leaves loose skin that can hang as an apron at the front or extend to the hips, lower back, and beyond.
Because abdominal muscle separation (diastasis recti) is often absent in this group, the choice of operation is largely determined by where your loose skin is located and how much there is. On examination, I assess the abdominal wall muscles for separation and perform abdominal muscle repair only where it is present. Where pregnancy has weakened the abdominal wall muscles, I assess the underlying muscles on their own merits.
Your weight should be stable first
 Do I Need After Weight Loss? Matching the Operation to Your Skin Pattern 3")
An abdominoplasty (tummy tuck) treats the skin you have now. It does not stop you gaining or losing weight later, and later weight gain or ongoing weight fluctuations can undo the result. For that reason, I prefer patients to be at a stable weight before surgery, with their weight loss largely settled rather than still actively dropping. Maintaining a healthy diet and regular exercise afterwards helps maintain the result.
If you are still losing weight, even with modern weight-loss medications, it is usually better to wait until things have levelled off. We can plan the timing together at the consultation.
Nutrition is part of the picture after weight loss
 Do I Need After Weight Loss? Matching the Operation to Your Skin Pattern 4")
Weight loss, whether through a weight-loss procedure such as bariatric surgery, through weight-loss medications, or through sustained dietary change, often leaves gaps in protein and other nutrient intake. Those gaps affect wound healing. This is why I assess nutritional status as part of deciding not just which operation to perform, but also when you are ready for it. I cover the preparation side further down.
Matching the operation to your skin pattern
Abdominoplasty procedures after weight loss are not all the same, and this is the part that matters most. Rather than starting with a procedure name, I start with where your loose skin sits and how far it extends. The operation follows from that.
Here is how I think about it.
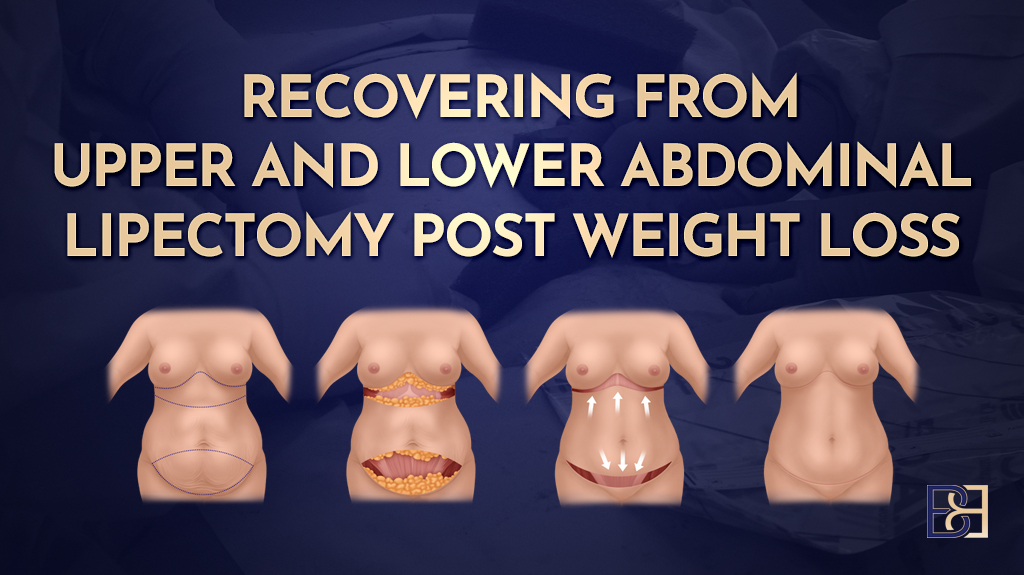
Loose skin mainly as a lower abdominal apron
 Do I Need After Weight Loss? Matching the Operation to Your Skin Pattern 5")
Some patients are left with a hanging fold of skin and tissue at the lower abdomen, often called an apron, while the skin higher up and around the sides is reasonably settled. Where the goal is to remove that overhanging skin, an apronectomy may be appropriate. This is a more limited operation that removes the apron of excess skin and fat, leaving the abdomen without the broader reshaping of a full abdominoplasty (tummy tuck). It can suit patients whose main concern is the apron itself, or whose health means a shorter operation is the better choice.
You can read more in my article on apronectomy after weight loss.
Vertical laxity across the front of the abdomen
 Do I Need After Weight Loss? Matching the Operation to Your Skin Pattern 6")
When the loose skin runs mainly up and down across the front, and there is enough of it to require repositioning of the belly button (umbilicus), a full or extended abdominoplasty (tummy tuck) is the usual answer. Through a low horizontal incision near the pubic hairline, I remove the excess abdominal skin between the belly button (umbilicus) and the pubic area, lift and redrape the upper skin, and bring the belly button (umbilicus) out through a new opening. The aim of this tummy tuck (abdominoplasty) surgery is to remove excess abdominal skin, resulting in a flatter stomach once the loose skin is gone. Where there is abdominal muscle separation (diastasis recti), I carry out abdominal muscle repair at the same time, though, as covered above, this is not a given after weight loss.
More details are in my guide to abdominoplasty after weight loss and bariatric surgery.
Both horizontal and vertical laxity
 Do I Need After Weight Loss? Matching the Operation to Your Skin Pattern 7")
After major weight loss many patients have loose skin in two directions at once. The skin is loose side to side, but also up and down, so that taking out a horizontal ellipse alone would leave the abdomen still loose. In that situation, a Fleur-de-Lis abdominoplasty allows skin to be removed in both directions. It adds a vertical line of excision to the horizontal one, which is what makes it possible to tighten the abdomen across and lengthwise. The trade-off is a vertical scar up the midline in addition to the low horizontal scar.
I describe how this operation is planned and performed in my step-by-step guide to Fleur-de-Lis abdominoplasty.
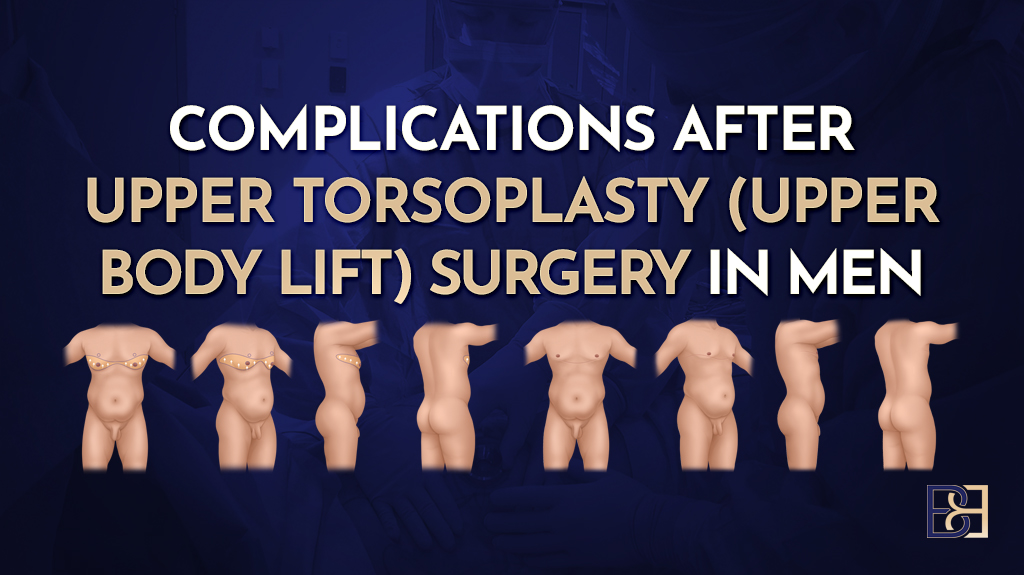
Loose skin that continues around the trunk
 Do I Need After Weight Loss? Matching the Operation to Your Skin Pattern 8")
For some patients, the loose skin does not stop at the front. The excess skin extends around the hips, flanks and lower back, so treating only the front would leave the rest untouched and create a mismatch. This is a larger surgical procedure than a front-only operation. Here, a body lift (belt lipectomy) treats the skin right around the trunk in a continuous band, lifting the front, sides and back together.
My article on belt lipectomy (body lift after significant weight loss) goes into this in more depth.
Combined patterns and my own approaches
Some skin patterns do not fall neatly into one of the above. Two approaches I use combine elements to treat multiple planes of laxity in a single operation.
- A dual vector abdominoplasty combines a Fleur-de-Lis with the removal of loose skin from the upper abdomen for patients with significant laxity both vertically and horizontally across the upper abdomen. It is not a smaller version of a Fleur-de-Lis. It treats more.
 Do I Need After Weight Loss? Matching the Operation to Your Skin Pattern 9")
- A circumferential hybrid abdominoplasty combines a body lift (belt lipectomy) with a vertical anterior excision, for patients who have both circumferential laxity and significant vertical laxity at the front.
 Do I Need After Weight Loss? Matching the Operation to Your Skin Pattern 10")
These are approaches I use when the pattern calls for them, as decided in the assessment. You can read about them in my articles on dual vector abdominoplasty and circumferential hybrid abdominoplasty.
What about a limited abdominoplasty (mini abdominoplasty)?
 Do I Need After Weight Loss? Matching the Operation to Your Skin Pattern 11")
A limited abdominoplasty (mini abdominoplasty), sometimes called a mini tummy tuck, is a smaller operation aimed at a small amount of loose skin low on the abdomen and is essentially a post-pregnancy procedure. After major weight loss, there is almost always more skin than a limited abdominoplasty can treat, so it is not an operation I use in this group.
Book your appointment online now
One operation, or staged across more than one?
A common question after weight loss is whether all the loose skin can be treated at once. Many of my patients want as much removed as possible in a single operation. Where someone is medically suited to it, that is often my preference too. It is a preference, not a rule, and whether it is right for you is worked out individually.
Why a single operation can make sense
Where a patient is suited to it, treating the loose skin in one comprehensive operation means one anaesthetic, one hospital admission, and one recovery to work through, rather than repeating each of those steps across two or three procedures. For the right patient, that is a genuine practical benefit.
Why staging is sometimes the better path
A larger operation is a bigger physiological event than a smaller one. For some patients, doing everything at once would place an excessive demand on the body. When that is the case, staging the work across separate operations is the more appropriate path. Staging is a legitimate clinical choice, not a lesser option and not a compromise. For some patients, it is the right approach, and I recommend it when it is.
The trade-off to weigh up
Consolidating the work into a single operation does not make the recovery any shorter or lighter in itself. A single comprehensive operation is a major event, and its recovery should not be underestimated. That is exactly why preparation before surgery carries more weight, not less, when a single larger operation is planned. Getting that preparation right is part of what makes a larger operation an appropriate choice in the first place.
How the decision is made
Whether one operation or staged surgery suits you is a clinical judgement made for you as an individual. It follows assessment of your medical history, your nutritional status, the pattern and extent of your loose skin, and what can be done well in a single operating time. We discuss it and decide it together at the consultation, not in advance.
What I assess at the consultation
 Do I Need After Weight Loss? Matching the Operation to Your Skin Pattern 12")
The consultation is where the operation is matched to you. A few things shape that decision.
Examining your loose skin
I assess the loose skin with you standing, because gravity shows the true pattern. I look at how much skin there is, where it sits, and whether it is loose in one direction or several. I check whether the laxity stops at the front of the abdomen or continues around the hips and back, since that is what separates a front-only operation from a body lift (belt lipectomy). I also look at the lower chest and the lateral thighs because loose skin there can influence how we plan and sequence things across the abdomen and beyond.
Previous abdominal surgery and existing scars
Earlier abdominal surgery matters. Previous abdominal surgery, including a caesarean, gallbladder surgery or bariatric surgery, leaves scars that can affect the blood supply to the skin and where incisions can safely be placed. I go through your surgical history and examine any existing scars when planning the incision.
Your general health
 Do I Need After Weight Loss? Matching the Operation to Your Skin Pattern 13")
Your medical history guides what is appropriate. Conditions such as diabetes and factors such as smoking affect wound healing and the risk of complications, so they feed directly into both the choice of operation and the decision between a single operation and staging. Smoking, in particular, has a strong effect on healing, and I talk this through with every patient.
Weight stability
 Do I Need After Weight Loss? Matching the Operation to Your Skin Pattern 14")
I check that your weight has settled. As covered earlier, an abdominoplasty (tummy tuck) treats the skin you have now, and large weight changes afterwards can undo the result, so a stable weight beforehand matters.
Nutritional status
 Do I Need After Weight Loss? Matching the Operation to Your Skin Pattern 15")
Most post weight loss patients have nutritional gaps that built up during weight loss. Before surgery, I arrange a blood panel to check protein status, iron studies, vitamin D and other markers, so that anything low can be corrected before theatre. This is part of deciding not only which operation to have, but also when you are ready for it. I cover preparation in more detail further down.
Adding liposuction (suction-assisted lipectomy)
 Do I Need After Weight Loss? Matching the Operation to Your Skin Pattern 16")
Patients often ask whether liposuction (suction-assisted lipectomy) can be combined with their abdominoplasty (tummy tuck). It can in selected cases, but its role after weight loss is usually smaller than people expect.
After major weight loss, the main problem is loose skin, not fat. Most of the abdominal fat has gone with the weight, so the operation is mostly about removing excess skin rather than removing excess fat from the tummy area. Where a localised pocket of fatty tissue remains that the skin excision alone will not treat, for example, at the flanks, liposuction (suction-assisted lipectomy) can be added to even out the contour.
I use liposuction (suction-assisted lipectomy) selectively alongside skin excision, in areas and amounts that do not compromise healing, rather than as a routine addition. VASER is one such technology; the principle is the same, whichever is used.
Whether liposuction (suction-assisted lipectomy) adds anything for you is assessed on examination, based on how much fatty tissue remains and where it sits.
Preparing well before surgery
 Do I Need After Weight Loss? Matching the Operation to Your Skin Pattern 17")
Good preparation matters more after weight loss, not less, and especially when a single larger operation is planned. A tummy tuck (Abdominoplasty) procedure after weight loss asks a lot of the body. Most post weight loss patients have nutritional gaps that built up while they were losing weight, and those gaps affect how well wounds heal.
Protein is the first thing I look at. Healing places a real demand on the body’s protein stores, and many patients are not meeting their daily protein target by the time they reach me. I assess this and work with you to lift it before surgery. There is more in my article on protein before and after abdominoplasty.
The pre-operative blood panel I arrange checks for the deficiencies that are common after weight loss, including iron, vitamin D, vitamin B12 and folate, so that anything low can be corrected ahead of time. I go through what to check and how to prepare in my nutritional checklist for abdominoplasty, as well as my overview of nutritional deficiencies after weight loss.
I work alongside your GP and, during your hospital stay, alongside the dietitian at Maitland Private Hospital, so your nutrition is supported through the whole period around surgery rather than only on the day.
Recovery and risks
Recovery from abdominoplasty surgery after weight loss takes time. A larger operation means a longer recovery, and it helps to be clear about what that involves before you decide.
Recovery realities
 Do I Need After Weight Loss? Matching the Operation to Your Skin Pattern 18")
- The hospital stay is usually a few nights.
- You will have drains in place for the first several days.
- A compression garment, sometimes called an abdominal binder, is worn for some weeks afterwards.
- Tight skin is common at first, along with changes in skin sensation around the scar, and these usually settle over time.
- Strenuous exercise is avoided for several weeks, then reintroduced gradually.
- Swelling settles gradually over months, not days.
- Most desk-based workers are back at work around four weeks. Manual workers usually need six to eight weeks.
- Scars are permanent. They fade and flatten over a year or more, but they do not go away.
Healing time and how your scars settle vary widely from one person to the next. A single comprehensive operation yields more of each of these than a smaller one, which is part of the trade-off covered earlier. I set out the timeline in detail in my article on recovery after abdominoplasty post weight loss.
Risks
 Do I Need After Weight Loss? Matching the Operation to Your Skin Pattern 19")
Every operation carries risk, and skin excision surgery after weight loss has its own pattern.
- Wound-healing problems, including wound infection, are more common in this group, partly because the nutritional gaps that weight loss can leave behind slow the healing process and partly because of the length of the incisions.
- A collection of fluid under the skin (seroma) can occur and may need draining.
- Blood clots in the legs (deep vein thrombosis, also called deep venous thrombosis) are a recognised risk of longer operations, which is why I assess and manage this for every patient. There is more in my article on DVT after body contouring.
- Thickened scars, or scars that widen, can occur.
- Smoking, diabetes and a longer operating time all raise these risks.
Serious complications are uncommon but possible, and the longer and more extensive the operation, the more some of these risks rise. That is one of the things weighed up when deciding between a single operation and staging the work.
Common questions
 Do I Need After Weight Loss? Matching the Operation to Your Skin Pattern 20")
How do I know which operation I need?
It is decided at your consultation. I examine your loose skin with you standing, look at where it sits and how far it extends, and take into account the amount of weight lost along with your medical history and nutritional status. The amount of skin removal that suits you follows from that.
Can all of the loose skin be treated in one operation?
For many patients, yes, where they are medically suited to it. For others, staging the work across more than one operation is the more appropriate path. Which applies to you is worked out individually at consultation.
Do I need muscle repair?
Not always. Muscle separation (diastasis recti) is more of a post-pregnancy issue, and many post weight loss patients do not have it. I check on examination and repair it only where it is present.
Will I have a vertical scar?
It depends on the operation. A full abdominoplasty (tummy tuck) leaves a low horizontal scar. A Fleur-de-Lis abdominoplasty adds a vertical scar up the midline, which is the trade-off for being able to remove loose skin in both directions.
Can I have liposuction (suction-assisted lipectomy) at the same time?
Sometimes. Liposuction (suction-assisted lipectomy) can be added when a pocket of fatty tissue remains, but its role after weight loss is usually limited, and it is used selectively to avoid compromising wound healing.
How much does it cost?
The cost of a tummy tuck (abdominoplasty) depends on the type of operation planned and your individual circumstances. I provide an itemised quote after your consultation, and there is more on my price list. Medicare and private health insurance sometimes cover part of the cost when eligibility criteria are met, and eligibility is assessed on a case-by-case basis.
When can I go back to work?
Most desk-based workers return after about 4 weeks. Manual workers usually need six to eight weeks. A larger operation can extend this.