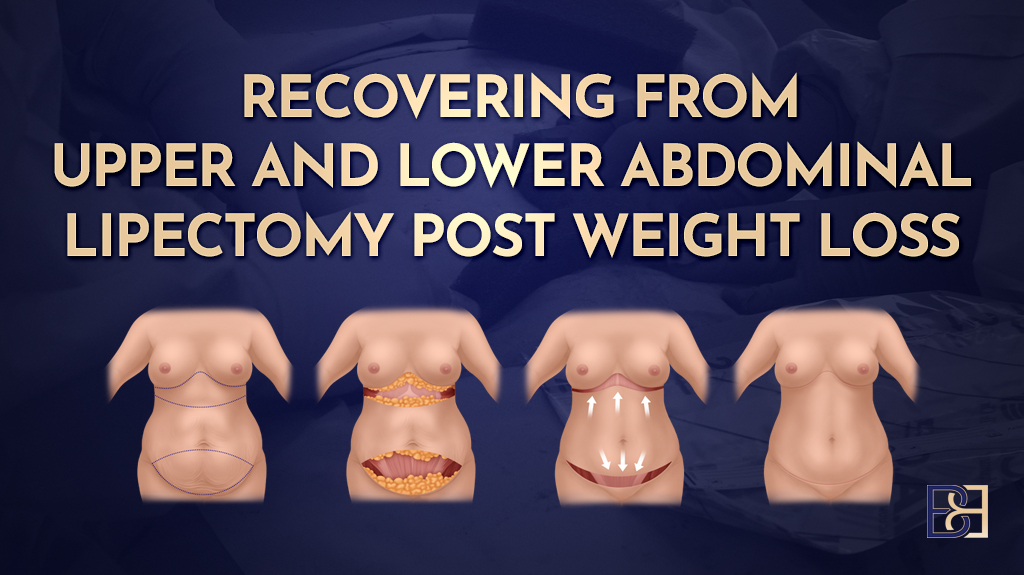
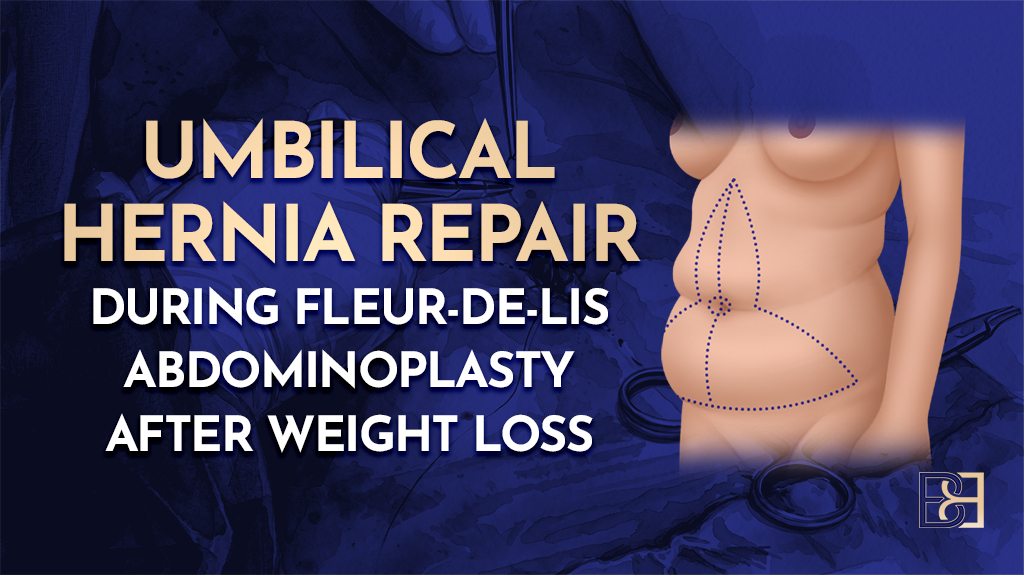
After major weight loss, the abdomen is often left with loose skin that hangs in both directions, down towards the pubis and across the waist. A standard tummy tuck (abdominoplasty) removes skin in one direction only, from top to bottom. For some post-weight-loss patients that is not enough. When there is significant width to take in as well as length, I use a fleur-de-lis abdominoplasty.
This article walks through that operation one step at a time, using photographs from a patient who came to me after losing 30 kg following gastric bypass surgery. Some of the images are graphic. I include them because I would rather you understand exactly what the operation involves before you decide whether it is right for you.
What a fleur-de-lis abdominoplasty does
 After Losing 30 kg of Weight: A Step-by-Step Operation Guide 1")
 After Losing 30 kg of Weight: A Step-by-Step Operation Guide 2")
The fleur-de-lis technique removes skin along two lines instead of one. There is the usual horizontal excision low across the abdomen, and a second vertical excision up the midline. Closing both pulls the remaining skin in from the sides as well as from above, which tightens the waist in a way a horizontal-only excision cannot. The trade-off is a vertical scar up the centre of the abdomen in addition to the horizontal one, leaving an inverted-T shape. The name comes from the fleur-de-lis, a stylised lily used in heraldry, which the incision pattern loosely resembles.
This is a bigger operation than a standard tummy tuck (abdominoplasty), and it is not the right choice for everyone who has lost weight. I only recommend it when the pattern of loose skin genuinely needs correcting in two directions. Whether it suits you is something I assess in person at consultation.
Where liposuction (suction assisted lipectomy) fits in
 After Losing 30 kg of Weight: A Step-by-Step Operation Guide 3")
Liposuction (suction assisted lipectomy) is not a routine part of this operation. Many post-weight-loss patients have very little fat left on the abdomen by the time they reach me, so there is nothing to suction. Where there is residual fat, usually around the flanks or the mons pubis, I may use liposuction as an adjunct within the same operation to refine the contour and to help free the loose skin. In this patient I used ultrasound-assisted liposuction, which uses sound waves to loosen fat before it is removed.
It is worth being clear about what this is and is not. The liposuction here is a step within the fleur-de-lis abdominoplasty, used selectively where it helps. It is not a second procedure added on for the sake of doing more.
Realistic expectations
Removing loose skin can relieve the functional problems that bring most of my post-weight-loss patients in, things like skin-fold rashes and difficulty with clothing and hygiene. What the operation cannot do is return the abdomen to the way it looked before weight gain. Skin that has been stretched and then deflated does not have its original elasticity, and scars are permanent. Results differ from one patient to the next depending on skin quality, the amount of loose tissue, body shape, and how the scars settle over time.
Getting your body ready before surgery
 After Losing 30 kg of Weight: A Step-by-Step Operation Guide 4")
A fleur-de-lis abdominoplasty is a larger physiological event than a standard tummy tuck (abdominoplasty), and that is exactly why preparation matters more, not less. Most people who reach me after major weight loss have nutritional gaps that built up while they were losing the weight, whether through bariatric surgery, weight loss medications, or sustained dietary change. Low protein and low levels of key vitamins and minerals all slow wound healing. A bigger operation asks more of the body, so I want those gaps corrected before I operate, not after.
Preparation starts at the first consultation. Every post-weight-loss patient has a comprehensive pre-operative blood panel ordered so we can see exactly where things stand, and I start a baseline supplement plan at the same time. I allow a minimum of four weeks of preparation before surgery, and longer where the bloods show a deficiency that needs correcting first. If protein stores or albumin are too low, I will delay surgery until they have improved, because operating into a nutritional deficit invites wound breakdown and infection.
I keep the detail of all this in separate articles rather than repeating it here. If you want to understand the nutrition side properly, start with my piece on protein before and after abdominoplasty, then the overview of nutritional deficiencies after bariatric surgery, and the vitamins and supplements hub. The blood tests themselves are covered in the pre-operative blood tests guide.
In the anaesthetic bay: markings and anaesthesia
 After Losing 30 kg of Weight: A Step-by-Step Operation Guide 5")
Before you go to sleep, I meet you in the anaesthetic bay to go over any last questions and to mark up your abdomen. This is also where you will meet your anaesthetist. Most of the anaesthetic assessment is done beforehand by phone, with the physical check, including your airway, carried out on the day.
Marking the excision
 After Losing 30 kg of Weight: A Step-by-Step Operation Guide 6")
The markings are my map for the operation. I draw them with an indelible marker while you are standing, because loose skin sits differently upright than it does on the operating table. I mark two main lines:
- A horizontal line running low across the abdomen from hip to hip, for the standard lower excision.
- A vertical line up the midline, for the central fleur-de-lis excision.
To judge the vertical excision, I draw the loose skin together from each side and see how much comfortably meets in the middle. That tells me how wide a strip I can remove without closing under too much tension. I mark both sides to match so the final result is as symmetrical as possible.
Anaesthesia
A fleur-de-lis abdominoplasty is done under general anaesthetic. The anaesthetist gives the medication through a drip, and once you are asleep a breathing tube is placed to manage your airway and breathing throughout. The anaesthetist stays with you for the whole operation, monitoring you from start to finish.
Freeing the belly button (umbilicus)
 After Losing 30 kg of Weight: A Step-by-Step Operation Guide 7")
Your belly button (umbilicus) is tethered deep down to the abdominal wall, a bit like the button on a tufted cushion. After major weight loss it is usually stretched and pulled downwards rather than sitting in a neat hollow, but it stays anchored on its stalk no matter how loose the surrounding skin becomes.
Because the fleur-de-lis removes a strip of skin straight up the midline, the skin immediately around the belly button has to come away too. So early in the operation I cut around the belly button to free it from that skin, leaving it attached to the wall on its stalk. The stalk itself is preserved.
I then mark the stalk so I can find it again once the central skin has been closed over the top of it. In this patient I used a small locating device on the stalk for that purpose. This matters because the area around the belly button is where some of the larger blood vessels pass up through the abdominal wall, and keeping track of the stalk helps me protect both the belly button and those vessels during the dissection that follows.
The vertical incision and central skin removal
 After Losing 30 kg of Weight: A Step-by-Step Operation Guide 8")
With the belly button (umbilicus) freed, I move to the vertical part of the operation. By this point we are in theatre and you are asleep. Working to the midline that was marked earlier in the anaesthetic bay, I incise along the central strip of skin to be removed. As I work I use diathermy to seal small blood vessels as they are cut, which keeps bleeding to a minimum.
The dissection carries down through the skin and fat to the firm abdominal wall beneath, and the loose midline strip is lifted away. I take care here not to injure the belly button stalk, which is why I marked and tracked it earlier. The area around the belly button is also where larger perforating vessels run up through the wall, so I work carefully through this zone.
 After Losing 30 kg of Weight: A Step-by-Step Operation Guide 9")
Where I have used liposuction (suction assisted lipectomy) earlier in the operation, it has already loosened the fat and reduced how much I need to cut by hand. Less dissection means more of the skin’s own blood supply, lymphatic drainage, and nerve supply is left intact, which supports healing and lowers the chance of wound problems (1).
Repairing muscle separation (diastasis recti), if it is there
 After Losing 30 kg of Weight: A Step-by-Step Operation Guide 10")
There is a common assumption that every tummy tuck (abdominoplasty) includes tightening the abdominal muscles. That comes largely from the post-pregnancy setting, where the two strips of the rectus muscle are often stretched apart down the midline. This gap is called muscle separation (diastasis recti), and it is measured as the distance between the muscle edges. A separation of more than about 22 mm above the belly button (umbilicus) is generally considered abnormal (2).
Post-weight-loss patients are different. Muscle separation (diastasis recti) is not a routine finding in this group, because weight loss does not stretch the abdominal wall the way pregnancy does. So I do not treat muscle repair as an automatic part of the operation. I assess each patient individually, and I only carry out a repair where there is a genuine separation worth correcting.
In this patient there was a separation, so I repaired it. With the abdominal wall exposed in the midline, I brought the muscle edges back together and stitched them, working in two layers with a strong, self-anchoring suture for a secure closure. Where there is no meaningful separation, this step is not needed, and adding it would lengthen the operation for no benefit.
Closing the vertical incision
 After Losing 30 kg of Weight: A Step-by-Step Operation Guide 11")
How the incision is closed has a lot to do with how the scar eventually settles. The midline is the part of this operation that closes under the most tension, because I am pulling skin in from both sides to narrow the waist. If that tension is allowed to fall on the skin itself, the scar tends to stretch and widen over time.
To avoid that, I close in layers. The deep layers do the heavy work, holding the two sides together and taking the tension off the surface. I use a strong anchoring stitch for these. The skin edges are then brought together with dissolving stitches placed underneath the surface, so there is nothing to remove later. I also bevel the edges as I excise, so the two sides meet cleanly and sit flat.
A vertical midline scar is the unavoidable trade-off of the fleur-de-lis technique, and it is permanent. It usually looks its most angry in the first few weeks, then fades and flattens gradually over a period that can stretch to two years. How a scar matures varies from person to person. I cover scar management and what to realistically expect in a separate article on fleur-de-lis abdominoplasty scarring after weight loss.
Removing the lower abdominal skin
 After Losing 30 kg of Weight: A Step-by-Step Operation Guide 12")
With the midline closed, I turn to the horizontal part of the operation, which is the same skin removal done in a standard tummy tuck (abdominoplasty). This deals with the apron of loose skin that hangs low over the pubis, the part most post-weight-loss patients are keenest to be rid of.
I lift the lower skin off the abdominal wall, working in a plane just beneath Scarpa’s fascia, a deep fibrous layer in the fat. Keeping that layer within the lifted skin helps protect its blood supply. The skin is then drawn downwards, the excess marked along the low hip-to-hip line, and that excess removed. The old opening where the belly button (umbilicus) used to sit is usually taken away with this lower skin.
Two things matter at this stage. The first is tension: I want the closure firm enough to hold the result but not so tight that it strains the wound or pulls the scar upwards. The second is symmetry, so the final horizontal scar sits level and as low as possible. As with the midline, I bevel the edges and close in layers, with the deep layer carrying the tension and dissolving stitches under the skin surface.
Book your appointment online now
Bringing out the belly button (umbilicus)
 After Losing 30 kg of Weight: A Step-by-Step Operation Guide 13")
The belly button (umbilicus) has been sitting on its stalk this whole time, attached to the abdominal wall and hidden under the skin I have just closed. The last main step is to bring it back out into its proper position.
Using the locating marker I placed earlier, I find the stalk and make a small opening in the overlying skin directly above it. I trim and shorten the stalk at its base and stitch it down, then bring it through the new opening and inset it with fine dissolving stitches around the rim. Shortening the stalk lets the belly button sit flush rather than protruding, and shaping the opening helps it look unobtrusive rather than round and obvious.
The belly button changes appearance over the first few months as swelling settles, and its final look, like the scars, takes time to reach. This is also why a stretched belly button after weight loss is very difficult to improve on its own. Without removing the surrounding loose skin, there is no good way to reposition it, which is part of why standalone correction of the belly button rarely makes sense in post-weight-loss patients.
Drains, dressings and compression
 After Losing 30 kg of Weight: A Step-by-Step Operation Guide 14")
Once everything is closed, I fit the drains, dressings and compression that you will go home with.
Drains
A fleur-de-lis leaves a large raw surface under the skin, and fluid collects there. To manage that I place two closed suction drains, one on each side, brought out through small exit points at the lateral hip. Each drain is a thin tube attached to a collection bottle that draws the fluid away by suction. I take the drains out once the daily output drops below a set level, which is usually somewhere between two and seven days. They often come out at different times, one before the other.
Dressings
 After Losing 30 kg of Weight: A Step-by-Step Operation Guide 15")
The incisions are covered with a PICO dressing, a single-use dressing that applies a small amount of negative pressure across the wound to help it heal. These stay on for the first week. At about day 7 they are removed and replaced with Hypafix, a soft adhesive tape worn over the scars.
Compression garment
 After Losing 30 kg of Weight: A Step-by-Step Operation Guide 16")
You will be put into a compression garment in hospital and I want it worn full-time for the first four weeks, then part-time for a further two weeks. Full-time means day and night, taking it off only to shower. The garment supports the tissues, helps control swelling, and reduces fluid build-up while everything settles. For the part-time fortnight, daytime wear is the priority, though there is some flexibility, for example overnight in hot weather.
Recovery: what to expect
A fleur-de-lis abdominoplasty is a major operation and the recovery is not something to underestimate. Here is what it generally looks like.
In hospital
 After Losing 30 kg of Weight: A Step-by-Step Operation Guide 17")
Most patients stay two to four nights. Pain is expected and is managed with medication, and the nursing team keeps an eye on your drains, your wounds and your general progress.
Getting moving early matters. I want you up and walking the day after your operation, even if only a few steps to start with. If walking is too much on that first day, the fallback is to at least get up and sit out of bed. Early movement lowers the risk of blood clots and helps your recovery along. You will be a little hunched at first because of the tightness across the abdomen, and that eases over the following weeks.
Back to everyday life
 After Losing 30 kg of Weight: A Step-by-Step Operation Guide 18")
- Lifting: nothing heavier than 10 kg until I clear you.
- Desk or sedentary work: usually around four weeks off.
- Manual or physical work: longer, generally six to eight weeks.
- Driving: once you are off strong pain medication and can move and brake comfortably, not before.
These are guides, not fixed dates. I give clearance to return to work and activity in person, and that can happen at any of your follow-up visits depending on how you are healing. I cover this in more detail in my article on returning to work after abdominoplasty, and exercise specifically in my article on exercise after abdominoplasty.
Follow-up
 After Losing 30 kg of Weight: A Step-by-Step Operation Guide 19")
I review you at four weeks, three months, six months and twelve months. The four-week visit is also when I hand your ongoing care back to your GP. Recovery is gradual, and while you will feel substantially better within the first couple of months, the scars and the final shape keep settling for up to two years.
If something does not seem right after hours
 After Losing 30 kg of Weight: A Step-by-Step Operation Guide 20")
If you have a concern outside clinic hours, call Maitland Private Hospital. The nursing staff run a phone triage and will advise you. If you need to be physically examined, go to your local emergency department. For anything life-threatening, such as chest pain or breathing difficulty, call 000. Maitland Private is not an emergency department, so please call ahead rather than presenting there unannounced.
Common questions
Is this major surgery?
Yes. A fleur-de-lis abdominoplasty involves general anaesthetic, removal of skin in two directions, often a muscle repair, a hospital stay of several nights and a recovery measured in weeks to months. It is a bigger operation than a standard tummy tuck (abdominoplasty), which is one reason I assess suitability carefully and put real effort into preparation beforehand.
Is liposuction (suction assisted lipectomy) always part of a fleur-de-lis abdominoplasty?
No. Liposuction (suction assisted lipectomy) is used selectively, where there is residual fat that needs refining or where loosening the fat helps free the skin. Many post-weight-loss patients have little fat left on the abdomen and do not need it at all. Whether it forms part of your operation is decided on your individual anatomy.
Will this tighten the skin on my back and flanks too?
Not on its own. A fleur-de-lis abdominoplasty treats the front of the abdomen and the waist. Loose skin that continues around the flanks and back needs a more extensive operation, such as a body lift (belt lipectomy), where the excision is carried right around the body. Whether that is appropriate for you is assessed at consultation. I cover it in my article on body lift (belt lipectomy) surgery after weight loss.
Is a fleur-de-lis abdominoplasty covered by Medicare?
Sometimes, in part. A Medicare rebate may apply for some post-weight-loss patients where specific medical criteria are met, for example documented problems with the overhanging skin. Eligibility is assessed individually and depends on your circumstances, not on weight loss alone. A GP referral is required, and I go through what does and does not apply to you at consultation.
References
- Saldanha OR, De Souza Pinto EB, Mattos WN Jr, Pazetti CE, Lopes Bello EM, Rojas Y, et al. Lipoabdominoplasty with selective and safe undermining. Aesthetic Plast Surg. 2003;27(4):322-327.
- Beer GM, Schuster A, Seifert B, Manestar M, Mihic-Probst D, Weber SA. The normal width of the linea alba in nulliparous women. Clin Anat. 2009;22(6):706-711.