Gynaecomastia, the enlargement of male breast tissue, is commonly classified into grades based on the severity of the condition. The appearance of enlarged breasts is a concern that affects males of all ages from puberty on.

Book your appointment online now
While the term “gynaecomastia” is frequently used as a blanket term when referring to male breast enlargement, some forms of this condition fall under the category of “true gynaecomastia” while others are considered “pseudo-gynaecomastia.”
True Gynaecomastia

True gynaecomastia is a condition characterized by the enlargement of breast tissue in males, which is caused by an imbalance between the hormones oestrogen and testosterone. Often seen during puberty, it can arise due to natural hormonal changes, certain medications, or underlying health conditions. While it is generally benign and may resolve over time, true gynecomastia can cause psychological distress and discomfort, prompting some individuals to seek medical evaluation and potential treatment options.
Pseudo-Gynaecomastia
In pseudo-gynaecomastia, the primary cause of enlarged male breasts is a buildup of fat that often manifests around, behind, or underneath the nipples. Although certain weight-lifting techniques and pectoral exercises can improve this condition by toning the chest, the most effective way to treat pseudo-gynecomastia is by removing fat via liposuction.
The vast majority of men with gynecomastia have both fat excess and excess glandular tissue in the breasts.
Determining the Best Approach with Gynaecomastia Surgery
Though gynaecomastia can be painful, the primary issues extend beyond the physical discomfort: reduced functionality, limitation on activities, and the emotional and psychological discourse that results. Treating this condition can vastly alleviate much of this emotional suffering, leading to ** body image.
Goals of Gynaecomastia Surgery
- Remove excess breast gland
- Eliminate loose skin and excess tissue
- Flatten and contour chest
- Create a masculine appearance

Tattoo blurred for privacy
Disclaimer: Operation performed by Dr Bernard Beldholm. Adult content, surgery has risks; individual results vary, seek 2nd opinion. Please see the full disclaimer.
Current Surgical Treatments
There are several advanced surgical techniques available for ** overdeveloped or enlarged breasts, each treating different aspects and severity of the condition. The most common procedures include:
1. Subcutaneous mastectomy
Mastectomy for gynaecomastia is a surgical procedure performed to remove glandular breast tissue from a male with enlarged breasts.
2. Liposuction
Liposuction is a popular choice for men with excess fat but minimal glandular tissue. This minimally invasive, and often preferred procedure for milder cases of gynaecomastia, involves suctioning out the fat to contour the chest, resulting in a more masculine appearance.
3. VASER Liposuction
A modern technique that utilises ultrasound technology to break down fat cells, making them easier to remove. VASER Liposuction is particularly effective for pseudo-gynaecomastia, where the enlargement is primarily due to excess fatty tissue rather than glandular tissue.
4. Combination VASER Lipo and Gland Excision
When both excess glandular tissue and fatty tissue are present, such as with massive weight loss patients, a combination of gland excision and VASER liposuction can provide the best results. Initially, VASER liposuction is performed to remove the surrounding fat. This is followed by the removal of excess breast gland tissue through a small incision in the areola.
5. Minor Skin Tightening Procedures
Minor skin tightening procedures such as the circular excision of skin and tightening as well as the different V lifts/U lifts are also used to treat male breast reduction.
6. Torsoplasty
Torsoplasty is a more extensive surgical option reserved for severe cases of gynaecomastia. This is a surgical procedure that involves removing excess breast tissue and repositioning the nipples to a more natural location on the chest.

Disclaimer: Operation performed by Dr Bernard Beldholm. Adult content, surgery has risks; individual results vary, seek 2nd opinion. Please see the full disclaimer.
Why Grading Systems Were Created
The grading systems outlined below were developed to help surgeons determine which approach is most appropriate for the patient in question. There are several grading systems that surgeons refer to when determining the best surgical approach for treating the condition, ranging from less invasive treatments like liposuction for lower grades to more complex procedures such as gynaecomastia surgery.
For a deeper dive into the gynaecomastia surgery journey, read my article, Essential Insights on Gynaecomastia Surgery for Men.
Many of the grading systems are old and outdated. Original systems put in place by Simon and Rodrich are not detailed enough
- Treatments have changed
- Patients have changed.
- More weight loss surgery patients experiencing loose skin after massive weight loss
- Obesity epidemic is causing more pseudo gynaecomastia cases than ever
- Changes in body acceptance and aesthetic goals
- Results based on these systems are not successful based on today’s standards.
The purpose of creating grading systems in gynaecomastia management was initially to provide a standardised way of assessing the severity of the condition, guide treatment decisions, and predict outcomes.
The thought was, by categorising gynaecomastia into different grades based on factors like breast size, skin excess, and degree of ptosis (**), healthcare providers can tailor treatment approaches more effectively. The hope was that a well-defined grading system would facilitate more effective communication among specialists and ensure that patients received consistent care.
Ultimately, an accurate grading system should aid in optimising surgical techniques and ** patient ** by setting realistic expectations.
Download our free guide: “Do I have Gynecomastia? Find out in 3 Easy Steps”

Evolution of Classification Systems for Gynaecomastia

Over the years, gynaecomastia classification systems have evolved from having a ** focus on breast size and skin excess (Nydick, et al, 1961) to more sophisticated models that integrate modern technique like VASER liposuction, accomodate the growing number of post weight-loss surgery patients, and acknowledge the importance of ** skin elasticity and quality, among other factors.
In 1961 when the Nydick Classification was developed, it was revolutionary, placing a focus on anatomical features like volume and excess.
When the Barros System was developed in 2012, a greater emphasis was placed on skin elasticity, making it more relevant for patients who lost a significant amount of weight.
Newer models, such as the Punia and Gupta System, refined the classification to ** hypertrophy and skin excess as well, also incorporating modern techniques such as VASER liposuction. A more patient-centric system, Punia and Guta recognized the importance of ** the physical and emotional impact this condition has on the patient.
By providing surgeons with more detailed guidelines for determining the appropriate treatment options, the more advanced systems are better equipped at helping doctors tailor treatments based on each patient’s unique presentation.
Why a One-Size-Fits-All Approach is Insufficient
The large quantity of grading systems for gynaecomastia reflects the complexity and variability inherent in this condition. Gynaecomastia, defined as the benign enlargement of male breast tissue, can manifest in diverse ways with varying degrees of severity. Below are the reasons why a one-size-fits-all approach is impractical.
Patient Diversity
Gynaecomastia can vary significantly in terms of volume and extent. Some patients may experience a minimal increase in breast tissue, while others face more pronounced growth that results in substantial physical and psychological discomfort. Consequently, different grading systems may place their emphasis on the volume of glandular tissue or the degree of ptosis, which is the ** of the breast tissue. Systems that prioritise these factors are essential for clinicians to accurately assess and select the appropriate surgical technique—ranging from liposuction to more extensive excisional surgeries.
Secondly, individual patient characteristics, such as skin elasticity, age, and the presence of excess adipose tissue, further contribute to the necessity of varied grading systems. For instance, older patients or those with significant weight fluctuations might exhibit different presentations compared to ** or leaner individuals. This variability necessitates systems that account for these distinctions, enabling personalised treatment plans that optimise outcomes and minimise complications.
Technological Advancements
Since the first grading system was developed in 1961, advances in medical technology and surgical techniques have introduced new variables that can influence treatment decisions, warranting evolving grading criteria.
As less invasive procedures and novel surgical approaches become more standard, grading systems must incorporate flexibility to adapt to these advances, ensuring that they remain relevant and applicable in modern practice.
Increase in Post-Bariatric Patients
There has been a significant increase in post weight loss patients with “pseudo-gynaecomastia” from loose hanging skin.
Cultural and Geographical Variables
Diverse cultural and regional perspectives on gynaecomastia treatment have contributed to variability in grading practices. Different regions may prioritise various aspects of the condition based on prevalent socio-cultural norms or available healthcare resources, leading to the development of region-specific grading criteria that may differ in focus and application.

Need for Universally Accepted System
The journey toward refining gynaecomastia treatment is ongoing, with each grading system derived from clinical experiences and outcomes. As new insights emerge, they highlight the dynamic and evolving understanding of this condition. Systems that integrate psychosocial components are particularly relevant, considering the significant impact gynecomastia can have on an individual’s mental health and quality of life.
Such systems not only ** physical correction but also incentivize comprehensive care that includes psychological support.
Overall, the multitude of grading systems for gynaecomastia highlights the individuality of each patient’s needs and the medical community’s commitment to providing tailored, effective care. As the understanding of gynaecomastia evolves, so too will the frameworks used to assess and treat it, ensuring they reflect both scientific advancement and the nuanced realities faced by patients around the world. Because these systems serve as crucial tools, allowing healthcare providers to more accurately convey the intricacies of gynaecomastia and select treatment plans that offer the best possible outcomes for patients, there needs to be a more universal system designed to bring all of the needs of the providers and patients in 2024.
The original systems put in place by Nydick, Simon, and others do not recognize the vast amount of causes and complexities of gynaecomastia grading. By examining all of these systems and taking into account the knowledge and experience Dr. Beldholm has acquired over the last 15 years, he is attempting to draw us closer to a universal categorization method that can become the gold standard for surgeons throughout the world.
Gynaecomastia Classification Systems (a Reverse Chronological Timeline)
Many websites and patient information resources provide information on grading systems and what treatments are available for patients. Some mention Grade II level patients requiring two treatments. For patients, however, it can be quite confusing as different websites present conflicting definitions, treatments, and outcomes for the various grades.
Some websites actually fail to mention the name of the grading system altogether.
To help clear up the confusion, Dr. Beldholm has carefully reviewed the original research reports for all grading systems that are available from the earliest to the present time.
He has also included the treatment recommendations written by each of the authors. It’s important to note that these are not Dr. Beldholm’s recommendations as several of these systems are outdated and no longer universally acceptable by the surgical community.
For the most up-to-date and comprehensive information about the grading systems, including those for pseudo and real post weight loss gynaecomastia, please refer to this article, Dr. Bernard Beldholm’s Grading System.
Historical Grading Systems (In Reverse Chronological Order)
Dr Beldholm Gynecomastia Grading System (2024)

Due to the limitations of the current grading systems, Dr. Bernard Beldholm combined the best of all of them and created his own guide, a comprehensive outline for treating gynaecomastia in the modern era, with modern treatments.
Dr Beldholm has developed the following grading system which includes the best of the aforementioned classification methods as well as his approach to treatments based on his 15 years of experience treating men with this condition.
Dr. Beldholm’s grading system for gynaecomastia helps determine the appropriate male breast reduction treatment for each patient.
Beldholm 2024 Grading and Treatment Recommendations
Gynaecomastia grade BB 1 (Mild)
Grade explained
- Small Gynaecomastia that is confined to within the areola, including “puffy nipple”
- Hard under the NAC (Nipple-Areola Complex), can usually be easily felt when palpated.
Treatment recommendation
- Subcutaneous mastectomy with infra-areolar incision
Gynaecomastia grade BB 2a (Moderate)
Grade explained
- Moderate gynaecomastia
- No ptosis
Treatment recommendation
- VASER liposuction
- Followed by subcutaneous mastectomy with an infra-areolar incision
Gynaecomastia grade BB 2b (Moderate to Severe)
Grade explained
- Moderate pseudo gynaecomastia
- No ptosis
Treatment recommendation
- VASER liposuction Only
Gynaecomastia grade BB 3a (Severe)
Grade explained
- Large gynaecomastia
- No ptosis
Treatment recommendation
- VASER liposuction
- Followed by subcutaneous mastectomy with supra-areolar incision
- Excision of skin above the NAC
Gynaecomastia grade BB 3b (Severe)
Grade explained
- Large pseudo-gynaecomastia
- No ptosis
Treatment recommendation
- VASER liposuction
- Followed by the excision of skin above the NAC
Gynaecomastia grade BB 4a (Severe with Ptosis)
Grade explained
- Gynaecomastia
- With ptosis
- NAC sitting 0-2 cm below the IMF
Treatment recommendation
- VASER liposuction
- Subcutaneous mastectomy with supra-areolar incision
- Excision of skin above the nipple to elevate NAC and remove loose skin
Gynaecomastia grade BB 4b (Severe with Ptosis)
Grade explained
- Pseudo-gynaecomastia
- With ptosis
- NAC sitting more than 2 cm below the IMF
Treatment recommendation
- VASER liposuction
- Excision of skin above the nipple to elevate NAC
Gynaecomastia grade BB 4c (Severe with Ptosis)
Grade explained
- Gynaecomastia (real or pseudo)
- With ptosis
- NAC sitting more than 2 cm below the IMF
Treatment recommendation
- Torsoplasty (upper thoracic lift) with free NAC
For a more in-depth examination of the Beldholm grading system, please refer to: Dr Beldholm’s 2024 Gynaecomastia Grading System with Recommended Treatment Options
Punia and Gupta Gynaecomastia Classification System (2023)

The Punia and Gupta classification is another classification method used to assess the severity of gynecomastia (enlarged male breast tissue). This system helps determine the best course of treatment based on the degree of tissue enlargement and cosmetic impact.
Building upon the Simon classification system, Punia and Gupta classification places more emphasis on skin redundancy and the degree of breast enlargement, allowing a more nuanced approach to treatment.
Placing a focus on breast enlargement and the presence of skin redundancy at different stages, Punia and Gupta Classification recognizes skin ** and excess at an earlier grade (Grade III), which is critical for deciding if the patient requires skin tightening along with tissue excision.
Punia and Gupta Gynaecomastia grades
Grade 1a: (Mild)
Grade explained
- Puffy nipple
Treatment recommendation
- Gland excision through an infra-areolar incision
Grade 1b: (Mild)
Grade explained
- Minor breast enlargement
Treatment recommendation
- Liposuction (around gland area) & Gland excision through an infra-areolar incision
Grade 2a: (Moderate)
Grade explained
- Moderate breast enlargement
Treatment recommendation
- Liposuction (around gland area & Axilla) & Gland excision & U skin lift from the supra-areolar approach
Grade 2b: (moderate)
Grade explained
- Moderate breast enlargement with ptosis
Treatment recommendation
- Liposuction (around gland area & Axilla) & Gland excision & U skin lift from the supra-areolar approach
Grade 3a: (large)
Grade explained
- Large chest enlargement with side rolls without ptosis
Treatment recommendation
- Liposuction (around gland area & Axilla) & Gland excision through an infra-areolar incision.
Grade 3b: (large)
Grade explained
- Large severe chest enlargement with side rolls with ptosis expected
Treatment recommendation
- Liposuction (around gland area & Axilla) & Gland excision & U skin lift from the supra-areolar approach
Grade 4a: (severe)
Grade explained
- Severe chest enlargement without significant ptosis
Treatment recommendation
- Liposuction (around gland area & Axilla) & Gland excision through an infra-areolar incision.
Grade 4b: (severe)
Grade explained
- Severe chest enlargement with significant ptosis. May need a second stage for tackling excess skin or same-stage axillary roles excision
Treatment recommendation
- Liposuction (around gland area & Axilla) & Gland excision & U skin lift from the supra-areolar approach.
- Second stage mastopexy may be needed.
Go to this article to find out more details about this grading system: Overview of Punia and Gupta gynaecomastia Classification system (2023)
Barros Gynecomastia Classification System (2012)

Proposed by Ana Paula Barros and colleagues to classify gynaecomastia based on the shape, size, and degree of enlarged breasts, as well as skin laxity (looseness), the Barros 2012 Gynecomastia Classification System is useful for ** surgical planning and guiding whether ** tissue removal or a more extensive surgical procedure is warranted. It also emphasises aesthetic outcomes and the degree of skin laxity in surgical planning.
Barros Gynecomastia grades
Grade I (Mild):
Grade explained
- Increased diameter & slight protrusion limited to the areolar region
Treatment recommendation
- Subcutaneous mastectomy through infra-areolar incision
- Liposuction is not required
Grade II (Moderate):
Grade explained
- Moderate hypertrophy of all the structural components of the breast, with the NAC above the inframammary fold
Treatment recommendation
- Liposuction is done first and then followed by removal of the breast gland through an infra-areolar incision
Grade III (Severe):
Grade explained
- Major breast hypertrophy, glandular ptosis and the NAC at the same height as or as much as 1 cm below the inframammary fold
Treatment recommendation
- Liposuction is done first and then followed by removal of the breast gland through an infra-areolar incision
- Donut Masopexy performed as part of the operation
Grade IV (Severe with Ptosis):
Grade explained
- Major breast hypertrophy, with skin redundancy, severe ptosis and the NAC positioned more than 1 cm below the inframammary fold
Treatment recommendation
- Reduction mammoplasty with superior or superior-medial pedicle
Go to this article to find out more details about this grading system: Barros Gynecomastia Classification System (2012) explained
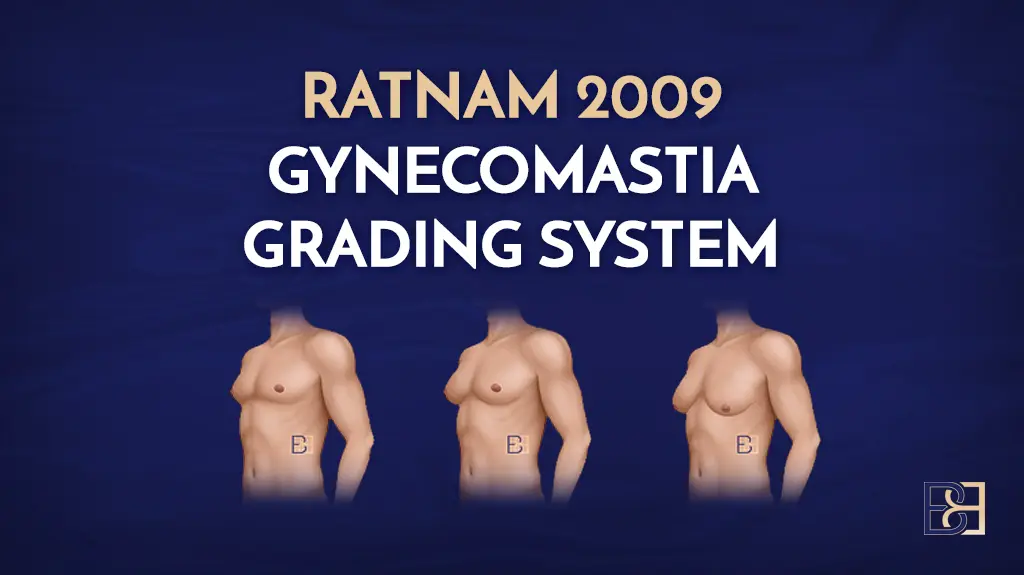
Ratnam Gynecomastia Classification System (2009)

Ratnam, B.V., 2009. A new classification and treatment protocol for gynecomastia. Aesthetic Surgery Journal, 29(1), pp.26-31.
The Ratnam classification system is practical for surgical planning, particularly as it highlights the need for skin excision and management of ptosis (**) as the grades increase.
Introduced by Chintamani Ratnam as a method to classify gynecomastia based on the amount of breast tissue, skin excess, and ptosis (**
), the Ratnam Gynecomastia Classification System helps in guiding the appropriate surgical treatment for male breast enlargement and is especially helpful in tailoring treatment for patients with significant ptosis and poor skin elasticity.
Ratnam Gynecomastia Grading
Grade I (Mild):
Grade explained
- Enlarged breasts with elastic skin & no fold
Treatment recommendation
- Subcutaneous mastectomy through an infra-areolar incision.
- Ultrasound-assisted Liposuction
Grade II (Moderate):
Grade explained
- Enlarged breasts with elastic skin & an IMF
Treatment recommendation
- Subcutaneous mastectomy through an infra-areolar incision followed by destruction of the Inframammary fold using a blunt liposuction cannula
- Ultrasound-assisted Liposuction of a wide area
- Followed by stimulation of the dermal surface of the breast skin by ultrasonic energy with 30% energy output for 3 minutes without using suction
Grade III (Ptotic breast):
Grade explained
- Ptotic breasts with inelastic skin
Treatment recommendation
- Subcutaneous mastectomy through an infra-areolar incision followed by destruction of the Inframammary fold using a blunt liposuction cannula.
- Ultrasound-assisted Liposuction of a wide area
- Followed by stimulation of the dermal surface of the breast skin by ultrasonic energy with 30% energy output for 3 minutes without using suction
- Reduction of the redundant skin sleeve by periareolar de-epithelialization and purse-string closure of the wounds around the areolae
For more details about this grading system, refer to this article: Ratnam 2009 Gynecomastia Classification System
Gusenoff Gynecomastia Classification System (2008)

Gusenoff, J.A., Coon, D. and Rubin, J.P., 2008. Pseudogynecomastia after massive weight loss: detectability of technique, patient ** , and classification. Plastic and reconstructive surgery, 122(5), pp.1301-1311.
Gusenoff Gynecomastia Grades
Grade 1a (Mild):
Grade explained
- No excess skin roll laterally
- Minimal excess skin and fat of the chest, with minimal alteration in nipple location and minimal descent of the inframammary fold
Treatment recommendation
- Liposuction (Ultrasonic liposuction was followed by suction-assisted lipectomy)
Grade 1b (Moderate):
Grade explained
- Lateral chest skin roll
- Minimal excess skin and fat of the chest, with minimal alteration in nipple location and minimal descent of the inframammary fold
Treatment recommendation
- Liposuction and direct excision of roll
Grade 2 (Moderate):
Grade explained
- NAC & inframammary fold below the ideal inframammary fold, lateral chest roll, and minimal upper abdominal laxity
Treatment recommendation
- Pedicled nipple reconstruction
Grade 3 (Severe):
Grade explained
- NAC & inframammary fold below the ideal inframammary fold, lateral chest roll, and significant upper abdominal laxity
Treatment recommendation
- Free-nipple graft reconstruction
Find out more about this classification system in this comprehensive article: Gusenoff Gynecomastia Classification System (2008).
Book your appointment online now
Cordova and Moschella Gynecomastia Classification System (2008)

Cordova, A. and Moschella, F., 2008. Algorithm for clinical evaluation and surgical treatment of gynaecomastia. Journal of plastic, reconstructive & aesthetic surgery, 61(1), pp.41-49.
Cordova Classification is based on the combination of tissue types (glandular and fat) and skin quality.
Cordova and Moschella Gynecomastia Grades
Grade I (Mild):
Grade explained
- Increase in diameter & protrusion limited to the areolar region
Treatment recommendation
- Subcutaneous mastectomy through an infra-areolar incision
- Liposuction is not required
Grade II (Moderate):
Grade explained
- Hypertrophy of all the structural components of the breast
- NAC is above the IMF
Treatment recommendation
- Ultrasound-assisted Liposuction is performed first
- Followed by subcutaneous mastectomy through an infra-areolar incision
Grade III (Large):
Grade explained
- Hypertrophy of all the structural components
- NAC at the same height as or about 1 cm below the IMF
- Include male tuberous breast
Treatment recommendation
- Ultrasound-assisted Liposuction is performed first
- Followed by subcutaneous mastectomy through an infra-areolar incision
- Followed by circular removal of skin around the NAC with round block suture
Grade IV (Severe):
Grade explained
- Hypertrophy of all the structural components, NAC more than 1 cm below the IMF
Treatment recommendation
- Central pedicle reduction mastoplasty techniques
- NO liposuction
Find out more about this classification system in this comprehensive article: Cordova and Moschella Gynecomastia Classification System (2008).
Rohrich Gynecomastia Classification System (2003)

Rohrich, R.J., Ha, R.Y., Kenkel, J.M. and Adams Jr, W.P., 2003. Classification and management of gynecomastia: defining the role of ultrasound-assisted liposuction. Plastic and reconstructive surgery, 111(2), pp.909-923.
A more nuanced classification system that accounts for the degree of skin excess and breast ptosis (drooping), the Rohrich classification is particularly useful in surgical planning.
This system is frequently used by modern plastic surgeons for patients with more advanced or complex cases of gynaecomastia.
Rohrich Gynecomastia Grading
Grade Ia
Grade explained
- Primarily glandular
- Minimal hypertrophy (<250g) with no ptosis
Treatment recommendation
- Ultrasound-assisted liposuction
Grade Ib
Grade explained
- Primarily fibrous
- Minimal hypertrophy (<250g) with no ptosis
Treatment recommendation
- Ultrasound-assisted liposuction
Grade IIa
Grade explained
- Primarily glandular
- Moderate hypertrophy (250-500g) with no ptosis
Treatment recommendation
- Ultrasound-assisted liposuction
Grade IIb
Grade explained
- Primarily fibrous
- Moderate hypertrophy (250-500g) with no ptosis
Treatment recommendation
- Ultrasound-assisted liposuction
Grade III
Grade explained
- Severe hypertrophy (>500g) with grade I ptosis
Treatment recommendation
- Ultrasound-assisted liposuction with or without staged excision
- (staged excision 6 to 9 months after liposuction)
Grade IV
Grade explained
- Severe hypertrophy with grade II or III ptosis
Treatment recommendation
- Ultrasound-assisted liposuction with or without staged excision
- (staged excision 6 to 9 months after liposuction)
Find out more about this classification system in this comprehensive article: Rohrich Gynecomastia Classification System (2003).
Cohen Gynecomastia Classification System (1987)

Cohen, I.K., 1987. Gynecomastia: suction lipectomy as a contemporary solution (Discussion). Plast Reconstr Surg, 80(3), p.386.
The Cohen Gynecomastia Classification System is one of the more straightforward systems, making it helpful for ** determining whether a patient requires skin excision or if they can be treated with less invasive techniques like liposuction or gland excision.
One of the earlier systems developed to assist surgeons in choosing appropriate treatment options for male breast enlargement, the Cohen 1987 Gynecomastia Classification System provides a concise way to classify gynecomastia based on the size of the breast tissue enlargement and the presence of excess skin.
Cohen Gynecomastia Grading
Group 1
Grade explained
- Predominantly Glandular
Treatment recommendation
- Open excision
Group 2
Grade explained
- Predominantly Glandular with ptosis
Treatment recommendation
- Open excision & liposuction. Sharp dissection to destroy Inframammary fold
Group 3
Grade explained
- Predominantly fat with some gland
Treatment recommendation
- Open excision & liposuction
Group 4
Grade explained
- Only fat
Treatment recommendation
- Liposuction only
Find out more about this classification system in this comprehensive article: Cohen Gynecomastia Classification System (1987).
Simon Gynecomastia Classification system (1973)

SIMON, B.E., HOFFMAN, S. and KAHN, S., 1973. Classification and surgical correction of gynecomastia. Plastic and reconstructive surgery, 51(1), pp.48-52.
One of the earliest systems created for classifying gynecomastia, the Simon Classification system primarily focuses on breast enlargement and the presence of skin excess.
Simon Gynecomastia Grades
Grade 1
Grade explained
- Small, visible breast enlargement – no skin redundancy
Treatment recommendation
- Subcutaneous mastectomy through an infra-areolar incision
Grade 2A
Grade explained
- Moderate breast enlargement without skin redundancy
Treatment recommendation
- Subcutaneous mastectomy through an infra-areolar incision
Grade 2B
Grade explained
- Moderate breast enlargement with skin redundancy
Treatment recommendation
- Subcutaneous mastectomy through a supra-areolar incision
- Excision of skin above areola in semi-circle
Grade 3
Grade explained
- Marked breast enlargement with marked skin redundancy i.e. pendulous female breasts
Treatment recommendation
- Excision of skin as well as glands
- Suggest staged approach
Find out more about this classification system in this comprehensive article: Simon 1973 Gynecomastia classification system.
Nydick Gynecomastia Classification System (1961)

Nydick, M., Bustos, J., Dale, J.H. and Rawson, R.W., 1961. Gynecomastia in adolescent boys. Jama, 178(5), pp.449-454.
Developed by Irving Nydick, the Nydick 1961 Gynecomastia Classification System, is a ** system based on the diameter of the breast tissue. As it was one of the earliest grading systems for male breast enlargement, this system primarily focuses on the size of the glandular enlargement without ** factors like skin excess or ptosis (**), making it far less detailed than the more modern classification systems.
Nydick Gynecomastia Grading
Grade 1
Grade explained
- Gland limited to the retro areolar region
- The gland does not reach the edge of the areola
Treatment recommendation
- Observation only. No treatment recommended
Grade 2
Grade explained
- The gland extends as far as the edge of the areola
Treatment recommendation
- Observation only. No treatment recommended
Grade 3
Grade explained
- Gland volume extends beyond the edge of the areola by no more than 5mm
Treatment recommendation
- Observation only. No treatment recommended
Grade 4
Grade explained
- Gland volume extends beyond the edge of the areola by more than 5mm
Treatment recommendation
- Observation only. No treatment recommended
Find out more about this classification system in this comprehensive article: Nydick Gynecomastia Classification System (1961)
Download our free ebook: “Gynaecomastia Surgery – Must know facts”

Dr Beldholm’s Final Thoughts

Gynaecomastia is a condition that occurs in men of all ages, causing a male chest to take on a female appearance, regardless of what the cause may be.
Important Factors to Consider
Real vs. Pseudo
From a surgical standpoint, when a patient presents with this condition, it doesn’t matter if the gynaecomastia is real or pseudogynecomastia, as the psychological impact is similar and can be quite frustrating to the patient. Therefore, I believe it is a mistake to limit a grading system to include only patients with a breast gland.
Presence of Breast Gland
In my experience, I have seen many post-weight loss patients with a significant amount of loose skin in the chest area with the appearance of female breasts. Though many do not contain breast gland tissue, as such, the impact is the same as if they did. For this reason, I have chosen to include patients with and without breast glands into my gynaecomastia staging system.
Patient Expectations
I place great emphasis on discussing risks, scars, and expectations with my patients during our initial consultation session.
With smaller grade gynaecomastia, the scars are placed in the areola and are usually well hidden. However with higher grades, when skin from the chest wall must be removed, there will be visible scarring.
I feel it’s important for the patient to be well-informed about what they can expect depending on the severity of their condition so they can make an educated decision. Patients must choose whether they are willing to accept having scars on their chest or would prefer to accept their current condition as it is. In other words, I discuss the trade-off.
It has been my experience that a majority of post weight-loss patients, after weighing all of the facts, are willing to accept having scars if it means they will have a flat, well-defined, masculine-looking chest again.
Each classification system helps to tailor the treatment plan to the severity of the gynaecomastia, balancing patient expectations with the extent of surgery required. While each method’s aim is to guide treatment options, they differ in their approach, focus, and criteria.
Many of the grading systems mentioned above involve the flattening of the inframammary fold. I believe, however, that varies from patient-to-patient and each individual case should be customised to suit the individual rather than proceed with a cookie-cutter approach
References
- Nydick, M., Bustos, J., Dale, J.H. and Rawson, R.W., 1961. Gynecomastia in adolescent boys. Jama, 178(5), pp.449-454.
- SIMON, B.E., HOFFMAN, S. and KAHN, S., 1973. Classification and surgical correction of gynecomastia. Plastic and reconstructive surgery, 51(1), pp.48-52.
- Cohen, I.K., 1987. Gynecomastia: suction lipectomy as a contemporary solution (Discussion). Plast Reconstr Surg, 80(3), p.386.
- Rohrich, R.J., Ha, R.Y., Kenkel, J.M. and Adams Jr, W.P., 2003. Classification and management of gynecomastia: defining the role of ultrasound-assisted liposuction. Plastic and reconstructive surgery, 111(2), pp.909-923.
- Cordova, A. and Moschella, F., 2008. Algorithm for clinical evaluation and surgical treatment of gynaecomastia. Journal of plastic, reconstructive & aesthetic surgery, 61(1), pp.41-49.
- Barros AC, Sampaio Mde C. Gynecomastia: physiopathology, evaluation and treatment. Sao Paulo Med J. 2012;130(3):187-97. doi: 10.1590/s1516-31802012000300009. PMID: 22790552; PMCID: PMC10876201.
- Ratnam, B.V., 2009. A new classification and treatment protocol for gynecomastia. Aesthetic Surgery Journal, 29(1), pp.26-31.
- Punia S, Gupta A. A New Clinical Classification for Gynecomastia Management and Predictive Outcome. Indian J Plast Surg. 2023 July 28;56(4):332-337. doi: 10.1055/s-0043-1770963. PMID: 37705810; PMCID: PMC10497332.
- Cohen KI. Discussion: Gynecomastia: suction lipectomy as a contemporary solution. Plast Reconstr Surg 1987;80:386.
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10497332/#JR2251755-2
- Nuzzi LC et al. “Psychosocial impact of adolescent gynecomastia: a prospective case-control study.”, Plastic & Reconstructive Surgery. 131(4):890-896, 2013 Apr.
- https://plasticsurgery.org.au/procedures/surgical-procedures/gynaecomastia
- https://my.clevelandclinic.org/health/treatments/24022-gynecomastia-surgery
- https://www.betterhealth.vic.gov.au/health/conditionsandtreatments/breast-reduction-for-men
- https://www.plasticsurgery.org/cosmetic-procedures/gynecomastia-surgery