Introduced in 1961, the Nydick 1961 Gynaecomastia Classification System focuses on identifying gynecomastia in its early stages, particularly in adolescents. Unique in its simplicity and practical focus on clinical assessment, Nydick is unlike later systems that categorize gynaecomastia into various stages based on the extent of breast enlargement and skin excess, which are more suited for advanced or adult cases.
A measurement-based system based on the assessment of breast tissue in adolescent males, using glandular tissue size as its criterion, the Nydick system’s uniqueness lies in its minimalist and early-stage focus, making it more applicable for certain clinical evaluations but less suitable for more advanced or aesthetically oriented cases.

Book your appointment online now
How Nydick Differs From Other Gynaecomastia Classification Systems
Defining gynaecomastia by the presence of palpable glandular tissue that is 2 cm or more in diameter beneath the areola, the Nydick system differs from other system as follows:
Emphasis on Palpable Glandular Tissue: Relatively straightforward for diagnosing gynecomastia in young males, the Nydick system uses glandular tissue size, setting a threshold of 2 cm, as its criterion.
Practical for Early Clinical Use: Introduced in the early 60’s, Nydick focuses on identifying gynaecomastia in its early stages, particularly in adolescents, unlike later systems that are more suited for advanced or adult cases and categorize the condition into various stages based on the extent of breast enlargement and skin excess.
Absence of Cosmetic or Severity-Based Staging: While other systems, like Rohrich and Simon, have introduced staging that considers aesthetic factors such as ptosis or the presence of excess skin, Nydick, which does not incorporate these elements, is less comprehensive, measurement-based, and purely anatomical.
Limited Use for Advanced Cases: The Nydick classification is a straightforward identification in early or mild cases and does not treat more severe gynaecomastia, where skin elasticity, breast size, and fat content vary significantly, as is common in older adult males.

Nydick Approach
Though, at the time of this study, it had been widely known that benign enlargement of the breast is a common occurrence in adolescent boys, the incidence of this condition had never been clearly defined and its cause and natural history had not been interpreted. Nydick sought to elucidate the following:
- Incidence of gynecomastia in normal young males of different ages, races, and complexions
- Characteristics and natural history of gynecomastia in young males
- How the occurrence of gynecomastia correlates with other physical changes in pubertal development

Materials and Methods Used
A majority of the boys in the study were 10 to 16 years of age, each attending a summer camp in New York State. Some of the participants were older boys working as camp counselors. Each boy had been initially examined by their family doctors, subsequently undergoing additional physical examinations by the participating examiners upon arrival and over a 3-year period.
Examiners gathered and recorded the following evidence:
- Height, weight, and age of each participant
- Amount of facial, axillary, pubic, trunk, and extremity hair
- Size of the penis and testes, each rated from 1 to 4+
- Thyroid size

Findings
A total of 2,369 examinations were performed on 1,890 presumably normal adolescent boys at a Boy Scout camp in New York State in an attempt to establish the incidence of pubertal gynecomastia and to correlate these findings with other factors in pubertal development.
The following observations were made:

Gynaecomastia was present in 38.7% of all examinations, with a peak incidence of 64.6% in the age group 14 years to 14 years and 6 months. It was unilateral in 23.3% of all cases of gynaecomastia.

- The condition persisted for up to 2 years in 27.1% and 3 years in 7.7% of boys examined.
- The 4 developmental features which appeared to be correlated most closely with the presence and size of gynaecomastia were size of testis, penis, and thyroid and amount of pubic hair.
- Though the authors suggested there might have been a relationship between gynaecomastia and certain hormones, they ascertained that such hypotheses would reveal too many inconsistencies.
- There was no apparent correlation with axillary, facial, trunk and body, or extremity hair.
- A gradual increase of 20% was observed in the 10-year-old boys; a 50% increase for 13 year-olds; and a peak of 64.6% at age 14.
- After age 15, the incidence appeared to drop dramatically to approximately 10%.
- Obese boys were excluded from the study because the authors felt their weight interfered with conducting an accurate assessment. Obesity was the basis for exclusion of 490 boys.
- Gynecomastia was diagnosed when a firm, discoid, sometimes tender subareolar nodule was present, with subareolar masses, and was rated on a scale of 1 to 4 plus.
The Nydick 1961 Gynecomastia Classification System has its own strengths and limitations, especially when compared to more modern and complex classification systems. Here’s a breakdown of its pros and cons:

Download our free guide: “Do I have Gynecomastia? Find out in 3 Easy Steps”

Nydick Gynaecomastia Classification System Advantages
- Simplicity and Ease of Use: The Nydick system relies on a single criterion (a palpable glandular tissue threshold of 2 cm under the areola), making it possible to apply without extensive training. It allows for straightforward assessment, which can be beneficial in busy clinical settings.
- Objective Measurement: By focusing on the presence of glandular tissue size (≥2 cm), it provides an objective standard that clinicians can easily measure, reducing subjectivity in diagnosis.
- Focus on Early Diagnosis: The system is particularly useful for diagnosing gynaecomastia in adolescents or in early stages, enabling early identification and monitoring for spontaneous resolution, which is common in pubertal gynecomastia.
- Practicality in Resource-Limited Settings: Without the need for imaging or additional classification criteria, the Nydick system can be applied in settings where resources for comprehensive assessments are limited.
Nydick Gynaecomastia Classification System Disadvantages
- Limited Scope: The Nydick system doesn’t account for the severity or progression of gynecomastia beyond the initial threshold. It lacks staging, which can be useful for determining the extent of the condition and guiding treatment decisions.
- Absence of Aesthetic Considerations: It doesn’t focus on factors such as breast ptosis), excess skin, or asymmetry, which are crucial in adult cases or in cases considering surgical intervention. Other systems, like the Simon or Rohrich classifications, take these into account and offer a more comprehensive assessment for cosmetic and reconstructive planning.
- Less Useful for Advanced or Severe Cases: The simplicity of the Nydick system makes it less suitable for cases where there is significant breast enlargement or skin excess. In such cases, other classification systems that consider the extent of tissue excess and skin laxity are more appropriate.
- Outdated for Surgical Planning: Since it was designed primarily for diagnostic purposes, it lacks the detailed staging necessary for contemporary surgical planning. Newer systems allow for tailored treatment plans based on the extent and nature of gynecomastia, while Nydick’s single-stage focus limits its utility in determining surgical approaches.
- Reliance on Palpation Alone: By focusing only on palpable tissue size, the Nydick system may not fully capture the condition’s complexity, especially in patients with a higher fat-to-glandular tissue ratio or pseudogynecomastia (fat-related breast enlargement without glandular involvement).
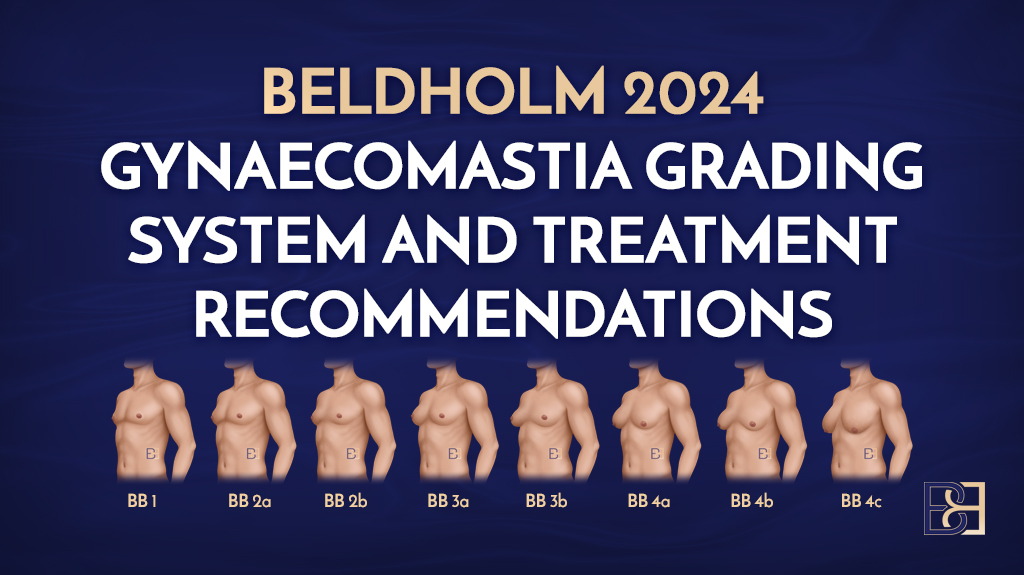
Nydick Gynaecomastia Classification System Grades

Grade 1: The gland is limited to the retroareolar region and does not reach the edge of the areola.

Grade 2: The gland extends as far as the edge of the areola.

Grade 3: The increase in gland volume extends beyond the edge of the areola by no more than 5mm.

Grade 4: The increase in gland volume extends beyond the edge of the areola by more than 5mm
*Observation only, no treatment suggestions included.
Summary of the Nydick Gynaecomastia Classification System
The Nydick 1961 Gynaecomastia Classification System uses a straightforward approach, making it useful for early or mild cases and in settings with limited resources. Its limited scope and lack of detail, however, make it less effective for advanced cases or modern surgical planning, where more complex and comprehensive staging systems may be needed.
The authors themselves concluded that there was a lack of conclusive evidence concerning the aetiology of gynaecomastia and a fuller understanding of the pathogenesis of pubertal gynaecomastia must await more intensive studies of the nature and order of evocation of the pituitary gonadotropins, the quantities and sources of androgens and estrogens, and the effects of temporary hormonal imbalances during adolescent development.
Dr Beldholm’s Overview of Nydick Classification System

From a historical perspective, I found this article to be very interesting as it tried to quantify the incidents of gynaecomastia. I found the study to be flawed in a number of ways, however.
First, it only explored the adolescent population in a very non-inclusive setting, as all the participants were healthy boys from middle class homes who were away at camp with the Boy Scout organization.
This is a very old study which makes it too primitive for modern applications, though it was very interesting.
The grading system for gynaecomastia is not useful for modern surgery or male gynaecomastia patients that I see in my clinic.
Grade 1-2 are basically small gynaecomastia that is treated with subcutaneous mastectomy.
Grade 3 basically groups together all of the other levels of severity and presentations, thus, not very helpful in modern practice.
Download our free ebook: “Gynaecomastia Surgery – Must know facts”

References
- Nydick, M., Bustos, J., Dale, J.H. and Rawson, R.W., 1961. Gynaecomastia in adolescent boys. Jama, 178(5), pp.449-454.